A nationwide study finds that most French adults fall short of optimal cardiovascular health, with marked differences by sex, education, and lifestyle, raising urgent calls for early, targeted prevention.
 Study: Life's Essential 8 cardiovascular health status of 18–69-year-old individuals in France. Image Credit: Cozine / Shutterstock
Study: Life's Essential 8 cardiovascular health status of 18–69-year-old individuals in France. Image Credit: Cozine / Shutterstock
In a recent article published in the American Journal of Preventive Cardiology, researchers investigated the distribution of the updated cardiovascular health (CVH) score based on recommendations from the American Heart Association among French adults. They identified important factors associated with having a higher score, including rural living (which was associated with higher scores, not lower, as sometimes assumed), fewer symptoms of depression, lower alcohol consumption, and higher educational attainment.
Background
Despite public health gains like smoking bans, cardiovascular disease (CVD) remains a leading global health burden, accounting for a third of deaths and significant disability. It is also a major economic burden, with estimates suggesting that it cost the European Union €282 billion in 2021, while only 3% of spending targets primary prevention. There is a growing need for primordial prevention, which focuses on preventing the development of risk factors to reduce the likelihood of cardiovascular disease (CVD).
To support this, the American Heart Association introduced tools to monitor CVH, including the Life's Essential 8 (LE8) – an updated score between 0 and 100 that includes sleep as a new health metric, alongside body mass index (BMI), activity, diet, blood pressure, blood glucose, smoking, and cholesterol.
A higher LE8 score is linked to reduced risk of CVD and other health outcomes. However, while LE8 scores have been assessed in the United States, little is known about their distribution in different countries or the factors that influence them.
About the Study
In this study, researchers estimated the distribution of LE8 scores and identified their determinants using data from a large, representative sample of French adults aged between 18 and 69, which was the primary analytic sample (though the original cohort included adults up to 75 years), collected between 2012 and 2019.
The LE8 score included eight components: blood glucose, blood pressure, cholesterol, sleep, BMI, nicotine exposure, physical activity, and diet. Diet was assessed using food frequency questionnaires, BMI based on measured weight and height, glucose, blood pressure, and cholesterol using clinical measurements, and sleep, smoking, and physical activity based on self-reported values.
Other data collected included family histories of cardiovascular disease (CVD), socioeconomic factors, depressive symptoms, use of alcohol, education, employment, cohabitation, sex, and age, as well as whether the respondent lived in a rural or urban area.
Each component was scored individually before averages were calculated. The researchers categorized the resulting scores as poor if they fell between 0 and 49, moderate for the range 50–79, and high for the range 80–100. For those on relevant medications, the research team deducted 20 points from their blood pressure or cholesterol scores. LE8 scores were standardized based on age before regression modeling was used to identify determinants.
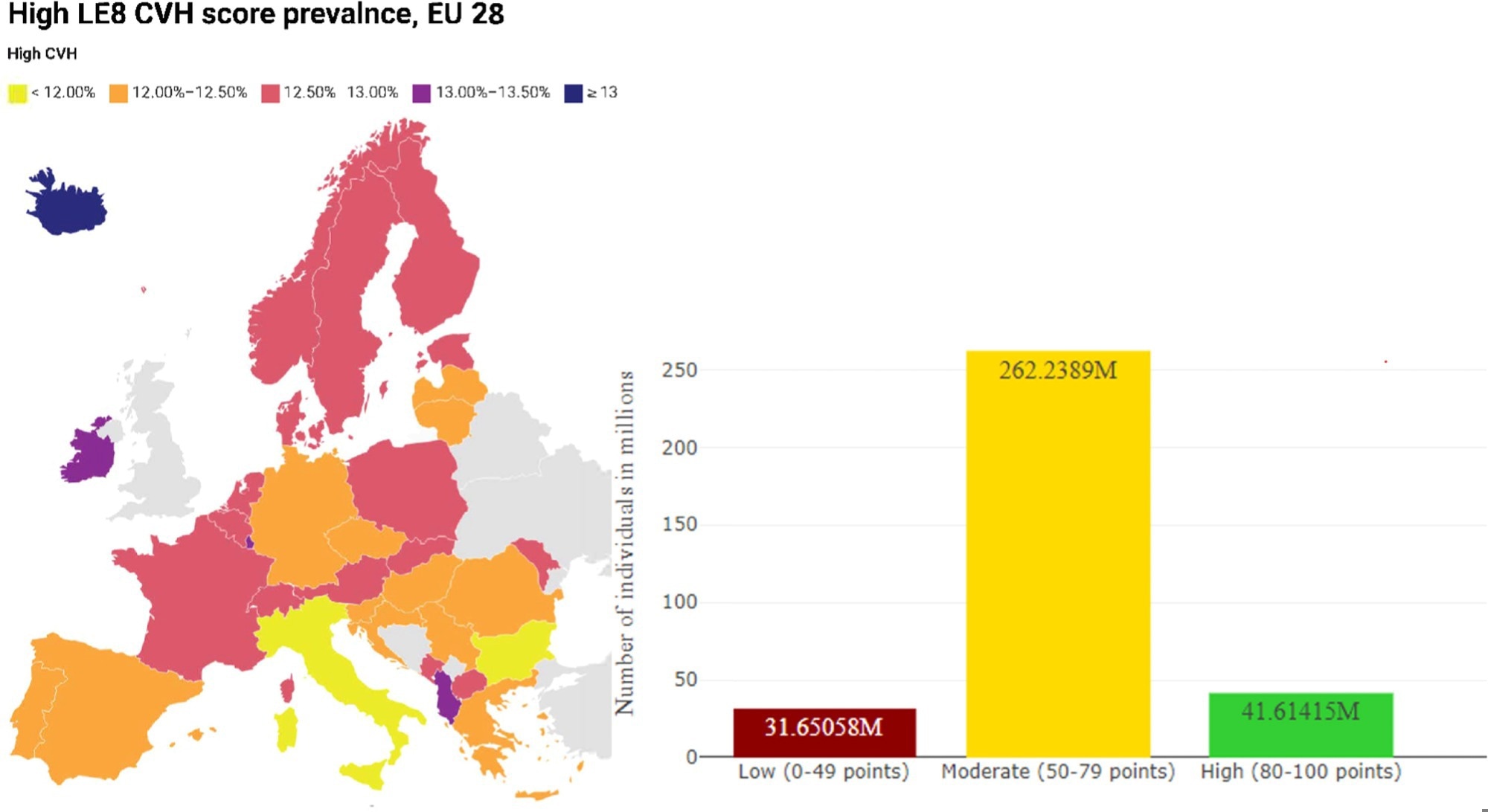
Age-standardized Life's Essential 8 score in EU 28 countries. Plot showing expected high CVH score prevalence (left panel) and distribution of low, moderate and high CVH scores in EU 28 (right panel). Life's Essential 8 score (LE8) ranges from 0 to 100 and is composed of eight cardiovascular health metrics: diet, physical activity, nicotine exposure, Body Mass Index, sleep health, blood glycemia, blood pressure, and blood lipids. LE8 CVH levels: Low LE8 (0–49 points), intermediate (50–79 points), and high (80–100 points). Age-standardized LE8 level prevalences and the expected number of individuals by CVH level were estimated using the EU 28 population as of January 1st, 2022.
Findings
The study analyzed data from 191,335 French adults without CVD, 54% of whom were female, with a mean age of 46.5 years. This represents around 45 million people between 18 and 69 in France.
The average LE8 cardiovascular health score was 66.1, with women scoring higher than men (68.9 compared to 62.8). The age-standardized LE8 score distribution showed that 12.4% had high scores, 78.2% moderate scores, and 9.4% low scores. When using weighted estimates, only 11.35% of adults met the threshold for high cardiovascular health, reflecting potential selection effects.
Educational attainment showed marked differences, as only 4.8% with less than a high school education had high LE8 scores, compared to 17.8% with two or more years of post-high school education. Rural residents actually had slightly higher cardiovascular health scores than urban residents, after adjustment for other factors, contrary to common assumptions. Notably, if all participants reached high LE8 levels, an estimated 81% of CVD events could be prevented.
The highest average metric was blood glycemia (95.5), and the lowest was diet (41.5). The consistently low diet scores for both men and women highlight a major public health challenge, as underlined by the study's authors. Men scored lower than women in most health factors, particularly blood pressure and BMI.
Higher LE8 scores were associated with being female, younger, well-educated, living in rural areas, employed in managerial roles, not cohabiting, and reporting fewer depressive symptoms, lower deprivation, and less alcohol consumption. Sensitivity analyses confirmed the robustness of these findings, though weighting slightly altered prevalence estimates.
The study also found that LE8 cardiovascular health scores decline progressively from age 18–20 up to about 55 years, then plateau, suggesting that age- and life-stage-adapted prevention strategies may be needed.
Conclusions
This is France's first nationwide LE8 analysis, revealing a lower prevalence of high CVH scores compared to the United States (13.2% versus 19.6%). Compared to findings from American populations, French adults had better physical activity, BMI, and glycemia scores, but worse sleep, blood pressure, and lipid levels.
Marked sex disparities were observed, with women nearly three times more likely than men to achieve high LE8 scores. The study’s strengths include its large, representative sample and detailed socioeconomic data. Limitations include reliance on self-reported data and cross-sectional design. The study was unable to fully assess all dietary components (e.g., sodium and fiber) and relied on self-reported HbA1c for most participants, which may limit the precision of some metrics.
The findings emphasize the need for targeted CVH interventions, especially for disadvantaged and male populations, and call for an intersectional approach to CVH promotion. The paper specifically notes the importance of considering complex and under-researched factors such as sexual minority status, as well as the need for interventions tailored to different population subgroups and life stages.
The authors also emphasize the importance of transitioning from a primarily care-oriented model to a more balanced approach that integrates both care and prevention, particularly primordial prevention, to enhance cardiovascular health at the population level.
Journal reference:
- Life's Essential 8 cardiovascular health status of 18–69-year-old individuals in France. Deraz, O., Kab, S., Touvier, M., Jouven, X., Goldberg, M., Zins, M., Empana, J. American Journal of Preventive Cardiology (2025). DOI: 10.1016/j.ajpc.2025.100981, https://www.sciencedirect.com/science/article/pii/S2666667725000534?via%3Dihub