Sponsored Content by AmplivoxReviewed by Maria OsipovaFeb 10 2025
Acoustic reflex tests assess intratympanic muscle response to elevated sound pressure. This measurement is performed using a tympanometer.
A survey carried out in 2012 by Emanuel et al. suggested that two-thirds of American audiologists include acoustic reflexes in their standard test battery.1

Image Credit: PeopleImages.com - Yuri A/Shutterstock.com
What is the acoustic reflex?
When a loud sound stimulus is presented to the ear, there is a reflexive contraction of the minute muscles that are connected to the ossicles in the Middle Ear. When these muscles contract, the stiffness of both the ossicular chain and the eardrum increases. However, it is widely accepted that the acoustic reflex in humans is "mainly, if not exclusively, [due] to [the] contraction of the stapedius muscle."2
The auditory activation of the tensor tympani muscle in humans occurs primarily as part of a startle response to extremely intense sounds. Acoustic reflex assessments can help in diagnosing:
- Conductive hearing loss
- Retrocochlear lesions
- Neurological disorders
How to perform acoustic reflex tests
An acoustic reflex test can be conducted either ipsilaterally or contralaterally. In both cases, a probe is placed in the ear canal to present a constant 226 Hz probe tone. Similar to tympanometry, this procedure measures changes in impedance within the middle ear system.
The peak pressure of the preceeding tympanometry test is applied during the Acoustic Reflex Assessment, whilst short (approximately 10 milliseconds) and loud test stimuli are presented to induce an impedance change due to the contraction of the stapedius muscle. Typical test frequencies are 500 Hz, 1 kHz, 2 kHz, and/or 4 kHz, with intensity levels ranging from 75 to 110–120 dB.
For ipsilateral testing, the test signals are delivered through the same ear where the probe is placed. For contralateral testing, a separate transducer delivers the test signals to the opposite ear. For example, if the probe is in the left ear and the transducer delivers the stimulus to the right ear, the test is contralateral.
It is important to note that different naming conventions exist for contralateral testing. According to the Aural Acoustic Immittance Standard (ANSI, 1987), contralateral refers to the ear receiving the stimulus (e.g., contralateral right: stimulus in the right ear, probe in the left ear).3
Other systems define contralateral based on the ear containing the probe (e.g., contralateral right: stimulus in the left ear, probe in the right ear). Amplivox tympanometers follow the latter convention.
The physiology of acoustic reflex measurements
Accurate interpretation of acoustic reflex measurements requires an understanding of the physiological processes within the acoustic reflex arc. This involves the coordinated actions of afferent and efferent neurons responding to external stimuli.
Afferent neurons carry sensory information from the ear to the central nervous system (the brain). In response, efferent neurons transmit signals from the central nervous system to muscles—in this case, the stapedius muscle—to execute a reflexive action.
Research indicates that the stapedius reflex is the primary sound-evoked pathway, making the behavior of the stapedius muscle the focus in this context.4
The auditory reflex arc is intricate. High-intensity stimuli reaching the cochlea activate the auditory nerve, which relays the information to the ipsilateral ventral cochlear nucleus (VCN).
From the VCN, the information is transmitted to the facial nerve nucleus, triggering motor neurons to activate the stapedius muscle. Simultaneously, the signal travels across pathways to the facial nerve nucleus of the contralateral ear, causing a contraction in the opposite stapedius muscle. This dual response underscores the complexity of the acoustic reflex arc.
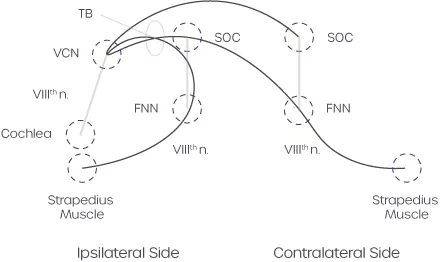
Figure 1. Schematic diagram of the crossed and uncrossed acoustic (straedius) reflex pathways. Abbreviations: FNN, facial nerve nucleus; SOC, superior olivary complex; TB, trapezoid body; VCN, venetral cochlear nucleus. Image Credit: Amplivox
The stapedius muscle contracts by pulling the stapes posteriorly, which stiffens the ossicular chain and moves the stapes away from the oval window. This action decreases middle ear admittance, a change that can be measured in the outer ear canal.
While the middle ear reflex pathway is often considered protective, studies have shown that it does not provide adequate protection against excessive auditory stimulation.5 However, the contraction of the stapedius muscle does produce frequency-dependent sound attenuation.6
This attenuation helps minimize the masking of speech frequencies by intense background noise, thereby preserving speech discrimination.7 Additionally, the stapedius muscle may contract to dampen internally generated vocalizations, reducing self-stimulation8
How to interpret acoustic reflex tests
Acoustic reflex measurements are typically conducted at frequencies of 500 Hz, 1 kHz, 2 kHz, and 4 kHz, assessed both ipsilaterally and contralaterally at varying intensities. In some cases, noise signals are also used, particularly when testing children.
Quick screenings often involve a single frequency and intensity, while diagnostic assessments include multiple sound levels to determine the full threshold profile.
Ipsilateral acoustic reflexes are usually measured at stimulus intensities ranging from 70 to 90 dBHL.9 Contralateral thresholds are typically 5 to 10 dB higher than ipsilateral thresholds. In addition to identifying the sound intensity at which the reflex occurs, the shape of the test curve provides critical insights into middle ear pathology.
This may include the deflection’s magnitude (e.g., 0.03 ml required), contraction time, and the degree of the curve gradient at both the start and end points. It’s recommended that a repeat presentation be conducted to verify the reflex threshold.
An overview of stapedius reflex threshold abnormalities is displayed below.10
Source: Amplivox
| |
Probe right |
Probe left |
|
| Ipsilateral |
Normal |
Normal |
Normal |
| Contralateral |
Normal |
Normal |
| Ipsilateral |
Abnormal |
Normal |
Afferent pathway lesion |
| Contralateral |
Normal |
Normal |
| Ipsilateral |
Abnormal |
Normal |
Efferent pathway lesion, i.e., middle ear abnormality or seventh-nerve paralysis (when the lesion is proximal to the innervation of the stapedius) |
| Contralateral |
Normal |
Abnormal |
| Ipsilateral |
Abnormal |
Normal |
Afferent pathway lesion i.e., eighth-nerve lesion with sufficient hearing impairment that the stapedius reflex cannot be elicited, i.e., vestibular neuroma |
| Contralateral |
Abnormal |
Normal |
| Ipsilateral |
Abnormal |
Abnormal |
Otosclerosis, i.e., mixed pattern |
| Contralateral |
Normal |
Abnormal |
| Ipsilateral |
Abnormal |
Abnormal |
Brainstem abnormalities, or bilateral middle ear disease |
| Contralateral |
Abnormal |
Abnormal |
Industry-leading tympanometers
Amplivox has worked hard to build industry-leading handheld and desktop tympanometers that offer fast and accurate middle ear assessments for all age groups, including neonates.
With a compact and elegant design that enables full portability, Amplivox’s tympanometers are perfect for mobile use and clinical environments where space is at a premium. With a broad spectrum of test functionality, Amplivox’s devices provide confidence that testing requirements are both met and surpassed.
References and further reading
- Emanuel, D.C., Olivia and Knapp, R.R. (2012). Survey of Audiological Immittance Practices. American journal of audiology, 21(1), pp.60–75. https://doi.org/10.1044/1059-0889(2012/11-0037).
- Gelfand, S.A. (2016). Hearing. CRC Press. 5th Edition https://doi.org/10.3109/9781420088663.
- American National Standards Institute (2020). ANSI/ASA S3.39-1987 (R2020) - American National Standard Specifications for Instruments to Measure Aural Acoustic Impedance and Admittance (Aural Acoustic Immittance). [online] Available at: https://webstore.ansi.org/standards/asa/ansiasas3391987r2020?srsltid=AfmBOoqmgmLIhfiFYpAU2q0RDZWlJG3o0z-dXYYGAPZd_OR5ysihFSN1 (Accessed 3 Jan. 2025).
- Borg, E. and Zakrisson, J. -e. (1974). Stapedius reflex and monaural masking, Acta Oto-Laryngologica, 78(1–6), pp. 155–161. https://doi.org/10.3109/00016487409126341.
- Aminoff MJ, Boller F, Swaap DF (2016). Handbook of Clinical Neurology | Elsevier. [online] Available at: https://www.elsevier.com/en-in/books-and-journals/book-series/handbook-of-clinical-neurology (Accessed 11 May 2024).
- Zakrisson, J.E., et al. (1980). Stapedius reflex in industrial impact noise: fatigability and role for temporary threshold shift (TTS). Scandinavian audiology. Supplementum, [online] (Suppl 12), pp.326–34. Available at: https://pubmed.ncbi.nlm.nih.gov/6939104/.
- Pang, X.D. and Peake, W.T. (1986). How Do Contractions of the Stapedius Muscle Alter the Acoustic Properties of the Ear? Lecture notes in biomathematics, [online] pp.36–43. https://doi.org/10.1007/978-3-642-50038-1_5.
- Borg, E. and Zakrisson, J.-E. (1975). The Activity of the Stapedius Muscle in Man During Vocalization. Acta Oto-Laryngologica, 79(3-6), pp.325–333. https://doi.org/10.3109/00016487509124694.
- Mrowinski, D. and Scholz, G. eds., (2006). Innentitel. Audiometrie. https://doi.org/10.1055/b-0033-4185.
- Aminoff MJ, Boller F, Swaap DF (2006). Handbook of Clinical Neurology | Elsevier. [online] Available at: https://legacyfileshare.elsevier.com/assets/pdf_file/0009/796482/0072-9752HBofClinicalNeurology_180611.pdf (Accessed 3 Jan. 2025).
About Amplivox
Amplivox creates a healthier future by providing accessible and accurate medical solutions for everyone.
As a manufacturer with more than 90 years of experience, we are proud to be a trusted partner to hearing and occupational health professionals all over the world by delivering a high level of knowledge-led solutions, service and support. We are here to be your preferred audiological and occupational health equipment provider.
Sponsored Content Policy: News-Medical.net publishes articles and related content that may be derived from sources where we have existing commercial relationships, provided such content adds value to the core editorial ethos of News-Medical.Net which is to educate and inform site visitors interested in medical research, science, medical devices and treatments.