An interview with Dr. Chris Subbe, Bangor University, conducted by April Cashin-Garbutt, MA (Cantab)
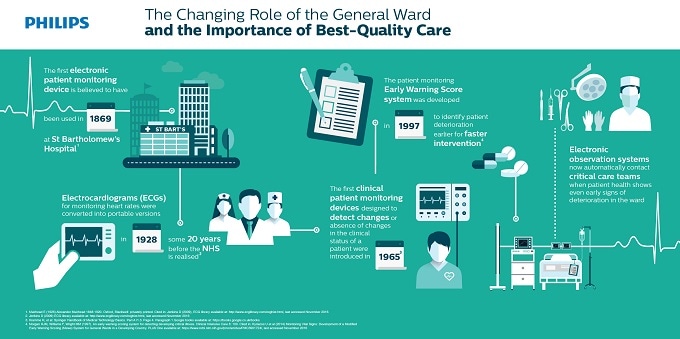
Vital signs have been around for a long period of time. Taking the pulse is probably one of the oldest examinations that doctors have made to assess patients.
When I first started, we would normally take the pulse, and maybe the blood pressure, and the temperature of a patient and we would write them down and chart them. Then saturations probes came along and people realized that measuring the speed of breathing is probably the most important thing, but it is also the most time consuming.
It is important how the individual signs come together. And, what I think has really made a difference, is being able to integrate these signs first into technological devices, and then secondly with Early Warning Scores, so that you can summarize all the information into a single figure.
Can you please outline Philips General Ward Solutions and explain how it integrates smart monitoring technology?
Philips General Ward Solution uses spot-check monitors, and gives them added value by giving them extra abilities and then integrating those into a larger system that allows to integrate complex information. This has several levels.
At the bedside level, the nurse will take the vital signs using a single device, which will also add value by calculating the degree of abnormality and personalising the assessment: Depending on what type of patient is being seen, the device will automatically correct for the underlying condition and is able to operate several scoring systems in parallel, and then would additionally give advice to you by issuing pre-programmed advice notifications on what to do with the score that comes out of that.
The second part is to make that information from the bedside, available to remote responders, for example the nurse in charge of the unit, a senior doctor, or someone from the Rapid Response Team, or in the UK the Critical Care Outreach Team. That's something that we've described as a "Triple Modular Redundancy".
This is a very crucial principle of safer systems and technology in the airline industry, or even working in computers. Several people hold on to safety critical information, and are able to make decisions based on that safety critical information. In my personal view, that is where the Philips General Ward Solution adds the most of the value.
 Credit: WHYFRAME/Shutterstock.com
Credit: WHYFRAME/Shutterstock.com
How is the Early Warning Score (EWS) calculated by the system and in what ways does this differ from the method that has typically been carried out in hospitals up until now?
The Early Warning Score is calculated from the raw data, for example, the speed of breathing, oxygen saturation, the concentration of inspired oxygen, blood pressure, heart rate, level of consciousness and temperature. Each of these modalities will be allocated values between zero and three points, depending on the degree of abnormality, and those will be added up and displayed as a single figure.
The difference between doing this on paper, and doing this within the Philips Solution is that it will be automatically calculated, and it will be calculated in the correct way.
We know that if people have to add up seven figures, there is a very high error rate in doing that. So, saying that someone is really quite ill and they got a score of six, if you calculate this by hand, and make a mistake this could mean that the patient is not escalated and this has significant safety implications.
In addition to this, users can personalise scores depending on what patient they are looking after. For example, a patient with a respiratory condition might need different weighting for those scores.
To operate several different systems in your head in parallel or even on paper is a real challenge. And, again, it means that the reliability of the assessments is reduced and that there is more chance of errors. So, that's another way how errors can be reduced through using these technological solutions.
What impact has the smart vital sign monitoring technology had on care so far?
The first impact is on the people who are working on the wards, who are the registered nurses and the health care assistants. We've had some very positive feedback from those teams, one comment being that the way in which the monitoring solution displays information is much clearer and is easier to process. And that's something that goes back to reducing cognitive load, not overburdening people who have to take complex decisions with information, but giving them the right information at the right time. That's at the user interface and then, the second part is, obviously, reduction in adverse events.
Did you see a reduction in the occurrence of serious adverse events at the original test site Ysbyty Gwynedd, the General Hospital in Bangor?
Yes, in our recently published VITAL II study, we compared two clinical areas before and after the implementation of the solution. We observed for a year without the additional monitoring and then for a further year with the additional monitoring, so overall, we had well over 4,000 patients in this study.
The events that we looked at were, cardiac arrests and unscheduled admissions into intensive care. We saw no increase in the number of patients who required intensive care, but these patients arrived in intensive care in a better condition, and had better chances to survive. The chance to survive with a better monitoring system was nearly twice as high.
With regards to cardiac arrest, we've seen a reduction in cardiac arrests from an already fairly low level by a further 80 percent. This illustrates the change in the way we're using data to change clinical outcomes.
What challenges still need to be overcome to improve vital sign monitoring further?
The big challenge that is right in front of us, is continuous monitoring. There are an increasing number of devices now that allow us to not just monitor vital signs every four hours, six hours, or twelve hours, but every five seconds or even every second. This produces a lot of data.
With that data, there will also be, false positives and false negatives. To integrate that into current work flows and extract only the safety critical information, is one of the toughest challenges ahead.
What do you think the future holds for early warning systems in hospitals?
There are some very exciting things ahead. At the moment, we're focusing mostly on vital signs, but we are collecting all sorts of information on hospitals, for example pathology data, data about renal function, bone marrow function, liver function etc., and that contains risk information. We're collecting this data repeatedly, so there's information about trends there.
We also know which patient gets which test, and how many tests they get. Patients who get more tests are usually sicker for example. There are big challenges and opportunities in integrating these complex data systems into single systems. Which is probably the biggest challenge is developing systems that summarize this information in the way that we can understand it quickly and draw the right conclusions from it.
To have the interface between technology and human in a way that it summarizes all the safety critical information and advises what, for that particular patient, is the individual and tailored right solution of further investigations and treatments.
Another thing that we're working on at the moment, that I think might change some of the drivers behind safety in hospital, is thinking about how patients could see some of the data that we're collecting and support safety systems.
So, if the patient would understand how ill they are, and what the conditions are that they're suffering from, they might be able to remind healthcare professionals to give them more information and they would be able to support their treatment in much better ways.
Patients could obviously hold their own monitors and use them at home already, so we would already know, when they come into hospital, what's normal for them. I think that's an area where a lot of things will happen in the next five years.
Where can readers find more information?
The VITAL II study has been published in Critical Care: https://ccforum.biomedcentral.com/articles/10.1186/s13054-017-1635-z
New edition of the textbook on Rapid Response Systems. There is also a lot of very interesting stuff by other people including more about what the challenges are to make hospital wards safer: https://link.springer.com/book/10.1007%2F978-3-319-39391-9
About Dr. Chris Subbe
Dr. Chris Subbe is a clinician working in Acute Medicine and lectures at Bangor University. He studied in Germany, where he also completed his MD in Respiratory Pathophysiology. He has trained in England, Germany and Wales and has complemented this with work for Medecins Sans Frontieres in Angola and fellowships in France and the US.
Dr. Subbe published the first peer-reviewed paper on Early Warning Scores and his research since focuses on collaborative working to create pragmatic solutions for practicing clinicians (http://www.ncbi.nlm.nih.gov/pubmed/?term=subbe).
He is co-founder of safer@home, the 1st international research collaboration in Acute Medicine and the Crisis Checklist Collaborative as an international patient safety group.
Dr. Subbe was recently appointed as an Improvement Science Fellow to the Health Foundation to examine the impact that patient contributions could make to safety in hospital.
 Menstrual blood HPV testing accurately detects cervical precancer
Menstrual blood HPV testing accurately detects cervical precancer