Researchers in the United Kingdom (U.K.) have observed substantially lower levels of anti-spike protein antibodies (anti-S) and subsequent higher risk of severe acute respiratory disease syndrome coronavirus 2 (SARS-CoV-2) breakthrough infections following the second dose of ChAdOx1 nCoV-19 (AstraZeneca/Oxford) vaccine as compared to BNT162b2 (BioNTech/Pfizer) vaccine.
 Study: Waning of SARS-CoV-2 antibodies targeting the Spike protein in individuals post second dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and risk of breakthrough infections: analysis of the Virus Watch community cohort. Image Credit: Kateryna Kon / Shutterstock.com
Study: Waning of SARS-CoV-2 antibodies targeting the Spike protein in individuals post second dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and risk of breakthrough infections: analysis of the Virus Watch community cohort. Image Credit: Kateryna Kon / Shutterstock.com
 This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Understanding the timeline of antibody waning is crucial
SARS-CoV-2 vaccines are designed to stimulate the production of antibodies targeting the spike protein of SARS-CoV-2. The level of antibodies following vaccination and trajectories of waning may differ between vaccines, thus influencing the level of protection, how soon protection is reduced, and, as a result, the optimum timing of booster doses.
The rate of deaths is substantially lower in vaccinated groups; however, 79% of recent coronavirus disease 2019 (COVID-19) deaths in the U.K. have occurred as a result of breakthrough infections in double vaccinated individuals at least 14 days prior to the positive SARS-CoV-2 test.
Given the high levels of breakthrough infections and subsequent deaths occurring in double vaccinated individuals, it is important to understand trajectories of anti-S waning in individuals after they have received their second dose of the COVID- 19 vaccine. Furthermore, it is important to determine whether the timing of their second dose can be used as a correlate of protection for SARS-CoV-2 infection in an effort to inform vaccine policies around the world.
How does antibody waning vary by vaccine type, demographic and clinical characteristics?
In the current study, anti-S levels were compared between ChAdOx1 and BNT162b2 vaccine recipients by time since vaccination, age, sex, and clinical vulnerability. A total of 24,049 samples from 8,858 individuals, 5,549 of whom received a second dose of ChAdOx1 and 3,205 received BNT162b2 vaccines, who remained anti-nucleocapsid (anti-N) antibody negative, were included in the analysis of anti-S waning over time.
Anti-S levels peaked following the second dose of vaccine and were nine-fold higher for BNT162b2 as compared to ChAdOx1. Later, waning anti-S levels followed a log-linear decline from three weeks after the second dose of vaccination.
At 20 weeks after the second dose of the vaccine, mean anti-S levels were 1521 U/ml for BNT162b2 and 342U/ml for ChadOx1 recipients. However, the overall rates of waning were higher in BNT162b2 recipients as compared to those who had received the ChAdOx1 vaccine.
There was no evidence of a difference in the rates of waning by age, sex, or clinical risk groups for BNT162b2 or ChAdOx1 vaccines.
Anti-S level, a meaningful correlate of protection against SARS-Cov-2 infection
In total, data from 8,275 individuals were analyzed for anti-S levels prior to breakthrough infection to examine anti-S as a correlate of protection against SARS-Cov-2 infection. Furthermore, these samples were also used to estimate a predicted time to reach a specified anti-S level for a threshold of protection. The team undertook survival analysis using a Kaplan-Meier descriptive analysis, in addition to a Cox regression model.
During the timeline for this particular study, the team observed 197 breakthrough infection cases. Further, they found that individuals with anti-S levels less than 500 U/ml following the second dose were nearly twice as likely to experience a breakthrough infection compared to those with higher levels.
Mean antibody levels declined to the threshold of 500 U/ml after about 3 months for ChAdOx1 and after about 7 months for BNT162b2. Thus, humoral protection wanes to levels associated with breakthrough infections before a 6-month period for those vaccinated with ChAdOx1 but not for BNT162b2.
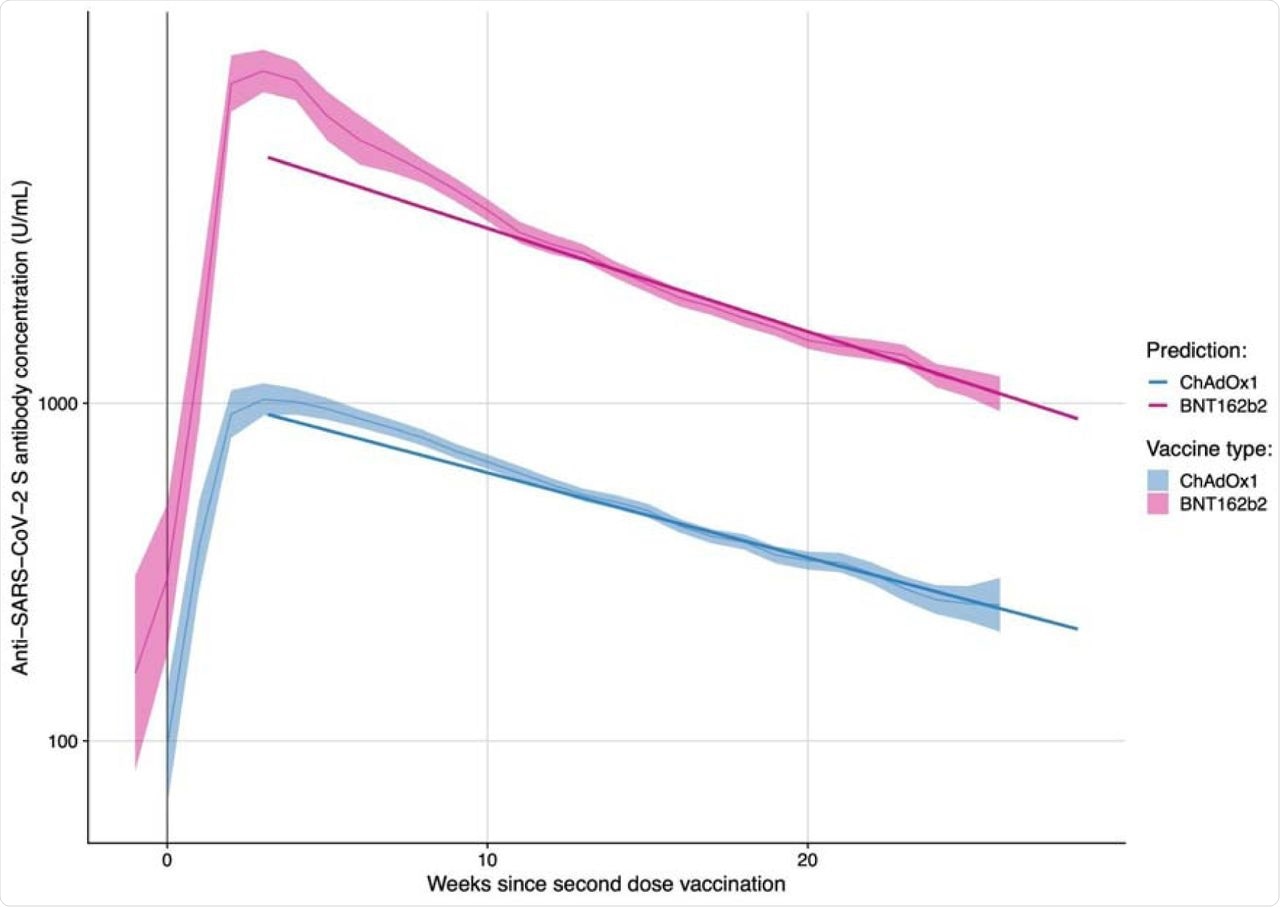 Anti-S levels (U/ml) over time since second dose of vaccination amongst N-seronegative individuals by vaccine type.
Anti-S levels (U/ml) over time since second dose of vaccination amongst N-seronegative individuals by vaccine type.
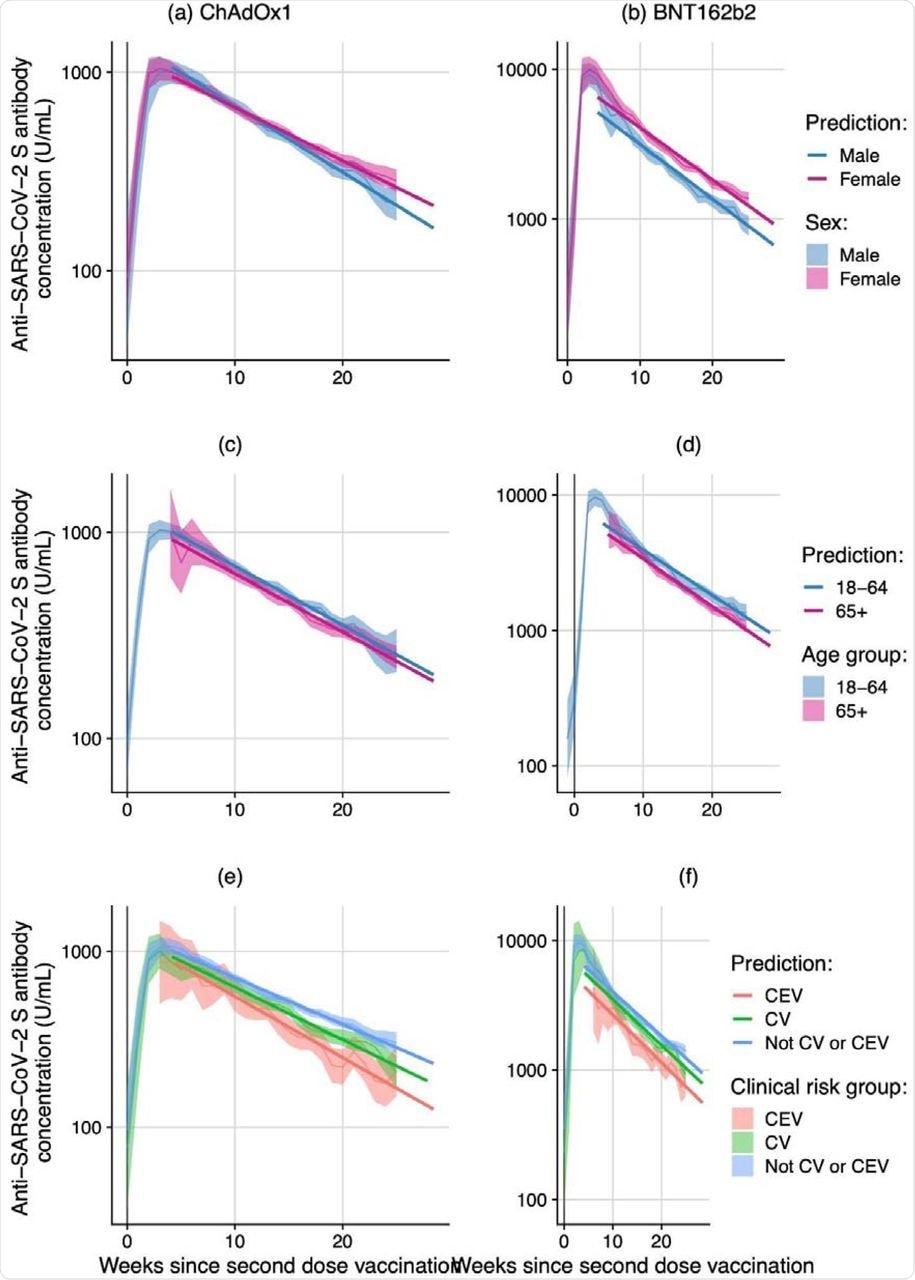 Anti-S levels (U/ml) over time since second dose of vaccination amongst N-seronegative individuals by vaccine type and sex, age and clinical risk group. (Note: Different y-axis scales for BNT162b2 and ChAdOx1)
Anti-S levels (U/ml) over time since second dose of vaccination amongst N-seronegative individuals by vaccine type and sex, age and clinical risk group. (Note: Different y-axis scales for BNT162b2 and ChAdOx1)
How does the vaccine type affect chances of breakthrough infection?
The current analysis included 14,340 participants who reported at least one test result in more than 14 days past the date of receiving their second vaccine dose or by the end of study follow-up.
The team found an increased risk of breakthrough infections for those who received the ChAdOx1 vaccine as compared to those who received the BNT162b2 vaccine. People vaccinated with ChAdOx1 had 1.43 increased odds of a breakthrough infection as compared to those doubly vaccinated with BNT162b2.
From 20 weeks onwards, the risk of breakthrough infection for BNT162b2 vaccinated individuals is approximately half of ChAdOx1. Furthermore, anti-S levels may provide an indication of the underlying correlates for this increased risk.
Nevertheless, circulating anti-S levels are unlikely to be the only immunological correlate of protection against COVID-19.Aas humoral immunity wanes, T-cell mediated immunity might act as the source of continued stable protection against infection and severe disease.
Noticeably, the timing of SARS-CoV-2 infections included in the current study coincided with the period when the Delta SARS-CoV-2 variant was the main circulating strain in England and Wales. Therefore, the team highlights that these findings may relate to many countries currently experiencing an increase in breakthrough infections due to Delta and where the populations have received ChAdOx1 or BNT162b2 vaccines.
“Together, these findings suggest that boosting ChAdOx1 earlier than six months after the second dose may be advantageous, particularly in those at greatest risk of severe outcomes.”
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Journal references:
- Preliminary scientific report.
Aldridge, R. W., Yavlinksy, A., Nguyen, V., et al. (2021) Waning of SARS-CoV-2 antibodies targeting the Spike protein in individuals post second dose of ChAdOx1 and BNT162b2 COVID-19 vaccines and risk of breakthrough infections: analysis of the Virus Watch community cohort. medRxiv. doi:10.1101/2021.11.05.21265968, https://www.medrxiv.org/content/10.1101/2021.11.05.21265968v1
- Peer reviewed and published scientific report.
Aldridge, Robert W., Alexei Yavlinsky, Vincent Nguyen, Max T. Eyre, Madhumita Shrotri, Annalan M. D. Navaratnam, Sarah Beale, et al. 2022. “SARS-CoV-2 Antibodies and Breakthrough Infections in the Virus Watch Cohort.” Nature Communications 13 (1): 4869. https://doi.org/10.1038/s41467-022-32265-5. https://www.nature.com/articles/s41467-022-32265-5.
 Griffith researchers on the cusp of new vaccine to prevent chikungunya
Griffith researchers on the cusp of new vaccine to prevent chikungunya