 *Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
In the United States and other nations around the world, a sharp increase in the number of pediatric SARS-CoV-2 infections and hospitalizations has been observed after the SARS-CoV-2 Omicron variant emerged. Studies conducted in the United Kingdom, South Africa, and Scotland have shown that hospitalizations driven by Omicron infections are comparatively lower than Delta infections. However, the clinical severity of COVID-19 in children has not been examined to date, which is critical given that kids under five years are currently ineligible for vaccinations.
About the study
In the present study, the researchers analyzed the electronic health records (EHR) of nearly 80,000 children in the U.S. who were infected by SARS-CoV-2 for the first time. The researchers included children who contracted COVID-19 during the dominant Delta wave, after the emergence of the SARS-CoV-2 Omicron variant, and just before the emergence of the Omicron variant when the Delta variant was still the major circulating variant.
The study population was stratified into three cohorts. The first Omicron cohort included 7,201 cases from December 9, 2021, to January 6, 2021, whereas the Delta cohort included 63,202 cases in the 10 weeks between September 1, 2021, and November 15, 2021. A second Delta cohort (Delta-2) with over 9,100 cases in the last two weeks of November 2021 was included in the current study.
The authors tested whether the clinical severity of COVID-19 differed in pediatric patients in the pre-and post- SARS-CoV-2 Omicron periods. Propensity-score matching was done for two cohorts including the Omicron and Delta cohorts and between two Delta cohorts.
Several were included in the score matching, of which included adverse socioeconomic health determinants like employment and education, the presence of medical conditions like cancer, influenza, asthma, and congenital heart disorders among others, as well as the use of COVID-19-related medications like remdesivir, dexamethasone, tocilizumab, and hydrocortisone.
Study findings
The researchers found that the average age of children in the Omicron cohort was lower than that of children in the Delta cohort. Racial and ethnic backgrounds varied between Delta and Omicron cohorts, and children in the Omicron cohort had fewer comorbid conditions and adverse socioeconomic health determinants.
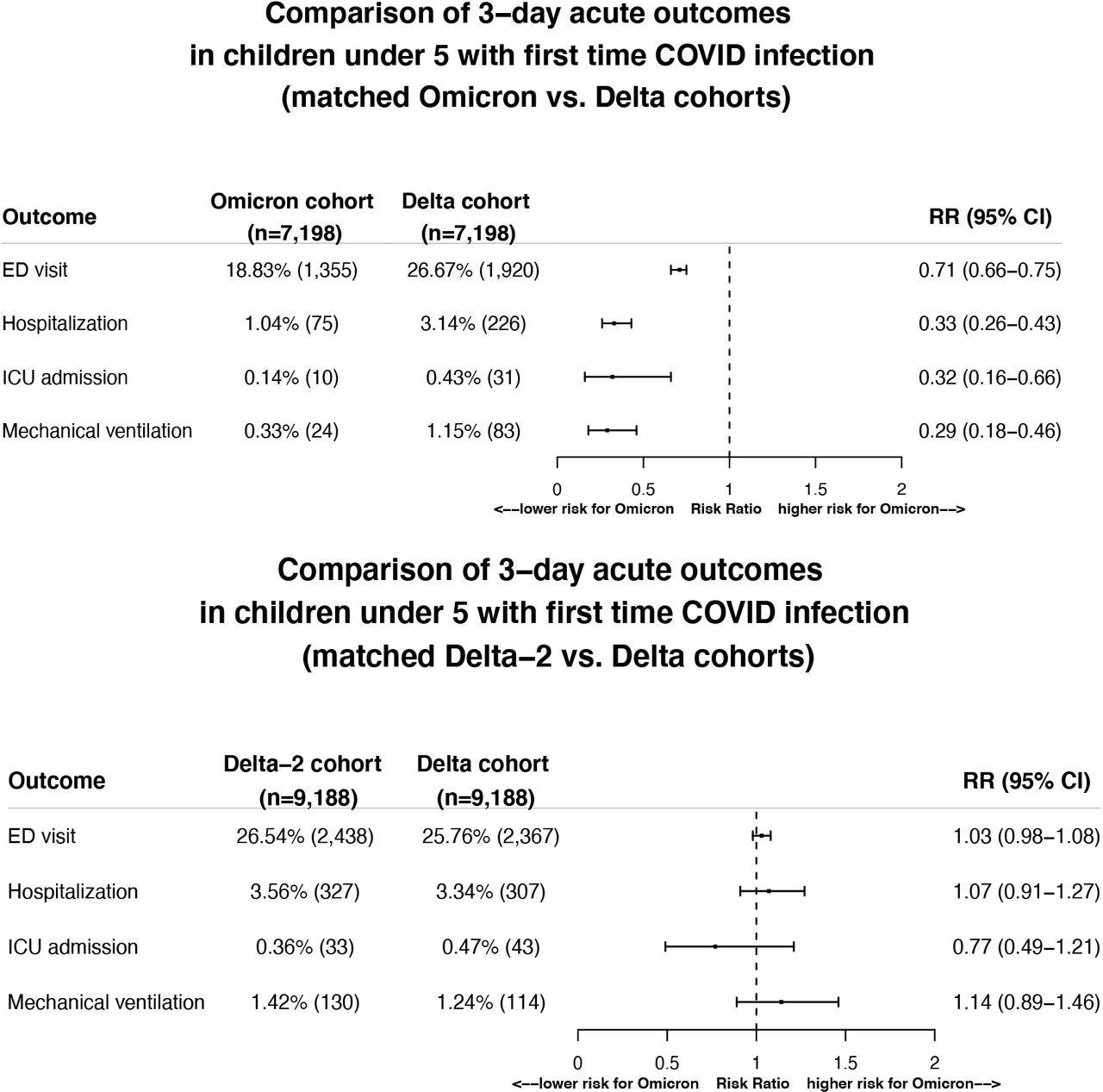
Comparison of severity of clinical outcomes including ED visits, hospitalizations, ICU admissions, mechanical ventilation in the 3-day time window that followed from the first day of SARS-CoV-2 infection between the matched Omicron and Delta cohorts (Top panel) and between the two matched Delta cohorts (Bottom panel). Omicron cohort – children under 5 who first contracted SARS-CoV-2 infection between 12/26/2021–1/6/2022 when Omicron was predominant and accounted for >92% of all variants circulating in the US. Delta cohort – children under 5 who first contracted SARS-CoV-2 infection between 9/1/2021–11/15/2021 when Delta was predominant and accounted for >99% of all variants circulating in the US. Delta-2 cohort – children under 5 who first contracted SARS-CoV-2 infection between 11/16/2021–11/30/2021, right before the Omicron variant emerged in the US and when Delta accounted for >99% of all variants circulating in the US. Cohorts were propensity-score matched for demographics (age, gender, race/ethnicity), socioeconomic factors, pediatric health conditions, and COVID-19 related medications.
As per EHR data between September 1, 2021, to January 6, 2022, 14.1% of the 520,624 pediatric cases who required medical attention were Black. During this same time period, over 26% of children in the Omicron cohort were Black as compared to 20% in the Delta cohort, thereby suggesting a disparity in COVID-19, even in pediatric COVID-19 cases.
The clinical severity of COVID-19 was assessed based on the number of visits to the emergency department (ED), hospitalizations, intensive care units (ICU), and requirement of mechanical ventilation within the first three days of a positive SARS-CoV-2 test. After the emergence of the Omicron variant, there was a drop in the number of ED visits, hospitalizations, ICU admissions, and mechanical ventilation support with risk ratios of about 0.71, 0.33, 0.32, and 0.29, respectively. No difference was observed in pediatric COVID-19 cases between the two Delta cohorts.
Conclusions
The findings of the present study noted the clinical severity of COVID-19 in children to be lower in those who contracted SARS-CoV-2 for the first time when the Omicron variant was dominant among other circulating SARS-CoV-2 strains. The adverse effects were also fewer for children in the Omicron cohort than those in the other two Delta cohorts.
A reduction of about 29% in the number of ED visits, 67% in hospitalizations, 71% in mechanical ventilation support, and 68% in ICU admissions within the initial three days of SARS-CoV-2 infection was observed for children in the Omicron cohort as compared to those in the Delta cohort.
Notably, the milder outcome of SARS-CoV-2 Omicron infection was not confounded by age, racial or ethnic composition, socioeconomic factors, and medications. The two Delta cohorts had similarities, thus suggesting that the disease severity of COVID-19 was not affected by factors like time, weather, and holiday seasons.
Furthermore, the current study was conducted on children below five years of age who contracted SARS-CoV-2 infection for the first time. Importantly, COVID-19 vaccines are currently unavailable to these children; therefore, they lack any pre-existing immunity. Altogether, these results suggest that COVID-19 caused by the SARS-CoV-2 Omicron variant leads to a milder clinical outcome in children under five years.
*Important notice: medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
 Specialized palliative care shows potential to enhance well-being in pediatric cancer patients
Specialized palliative care shows potential to enhance well-being in pediatric cancer patients