Growing evidence supports the fact that SARS-CoV-2 infections can lead to persistent recurrence of a wide range of COVID-19 symptoms. These sequelae, collectively known as PASC or >long coronavirus disease (long COVID), include post-exertional malaise, shortness of breath, neurological impairments such as difficulty concentrating, and numerous symptoms affecting almost every organ system. These symptoms also impact the overall quality of life.
Although some studies have found a decrease in PASC symptoms one year after recovering from the initial SARS-CoV-2 infection, among individuals with severe COVID-19 requiring hospitalization, these symptoms have been found to persist beyond two years.
Furthermore, studies have reported that a quarter of the cumulative disease and disability burden associated with PASC is from the second year after the initial infection. However, follow-up data beyond two years are limited, and the risks of persistent PASC symptoms or emergence of new PASC-associated risks in the long term remain unclear.
About the study
In the present study, the researchers used the health database of the United States Department of Veterans Affairs to examine a cohort of over 135,000 veterans who had recovered from SARS-CoV-2 infections and compared them to a larger cohort of over 5,200,000 individuals who had no history of COVID-19.
This three-year follow-up study enrolled participants from March to December 2020, when the dominant variant of SARS-CoV-2 was the ancestral strain, and no effective antivirals or COVID-19 vaccines had yet been developed. The researchers followed the two cohorts longitudinally for three years to estimate mortality risk and incident PASC across hospitalized and non-hospitalized COVID-19 patients.
To obtain long-term follow-up data, the electronic medical database containing detailed information on outpatient and inpatient hospital visits, laboratory test results, and prescription history of routine medical visits was used.
A list of 80 well-characterized COVID-19 sequelae, defined using International Statistical Classification of Diseases Tenth Revision codes, laboratory tests, and medical prescriptions, was used to determine the outcomes. Incident outcomes were those that did not occur in the two years preceding the positive SARS-CoV-2 diagnosis and whose first appearance was a month or more after the positive SARS-CoV-2 test result.
The outcomes were categorized into ten groups based on the impacted organ system, including pulmonary, neurological, musculoskeletal, metabolic, mental health, renal, gastrointestinal, fatigue-associated, cardiovascular, and coagulation. The study also calculated the disability-adjusted life years (DALYs) for the cumulative disease burden of the sequelae and their impact on overall health.
A set of covariates, including demographic characteristics such as sex, age, race, smoking status, and area of residence, and other covariates such as body mass index, glomerular filtration rate, and diastolic and systolic blood pressure, were considered potential confounders.
Additionally, comorbidities such as chronic lung disease, cardiovascular disease, anxiety, depression, dementia, chronic kidney disease, cerebrovascular disease, diabetes, peripheral artery disease, and an immunocompromised status associated with organ transplantation, cancer, human immunodeficiency virus, or the use of immunosuppressants or corticosteroids were also included.
Results
The study found that among individuals who had recovered from COVID-19 and had not required hospitalization, the mortality risk was no longer significant one year after the initial SARS-CoV-2 infection. The risk of PASC symptoms was found to have decreased in the three years following the initial SARS-CoV-2 infection but was responsible for 9.6 DALYs per 1000 persons in the third year following the infection.
For individuals who required hospitalization due to acute COVID-19, the mortality risk remained elevated despite undergoing a significant decline over three years. Similarly, the risk of incident PASC symptoms was also found to decline significantly over three years and yet contribute 90 DALYs per 1000 persons.
The mechanisms behind the increased risk of mortality or incident PASC symptoms for individuals with acute COVID-19 requiring hospitalization remain unclear. However, as reported by various previous studies, the researchers believe this increased risk could be due to underlying medical or genetic conditions or comorbidities that make certain individuals vulnerable to more severe forms of COVID-19.
The acute SARS-CoV-2 infection then leads to the replication of the virus in regions outside the pulmonary system and the persistence of the viral ribonucleic acid (RNA) in various regions of the body, resulting in a recurrent activation of the inflammatory and immune responses, which could be responsible for PASC symptoms.
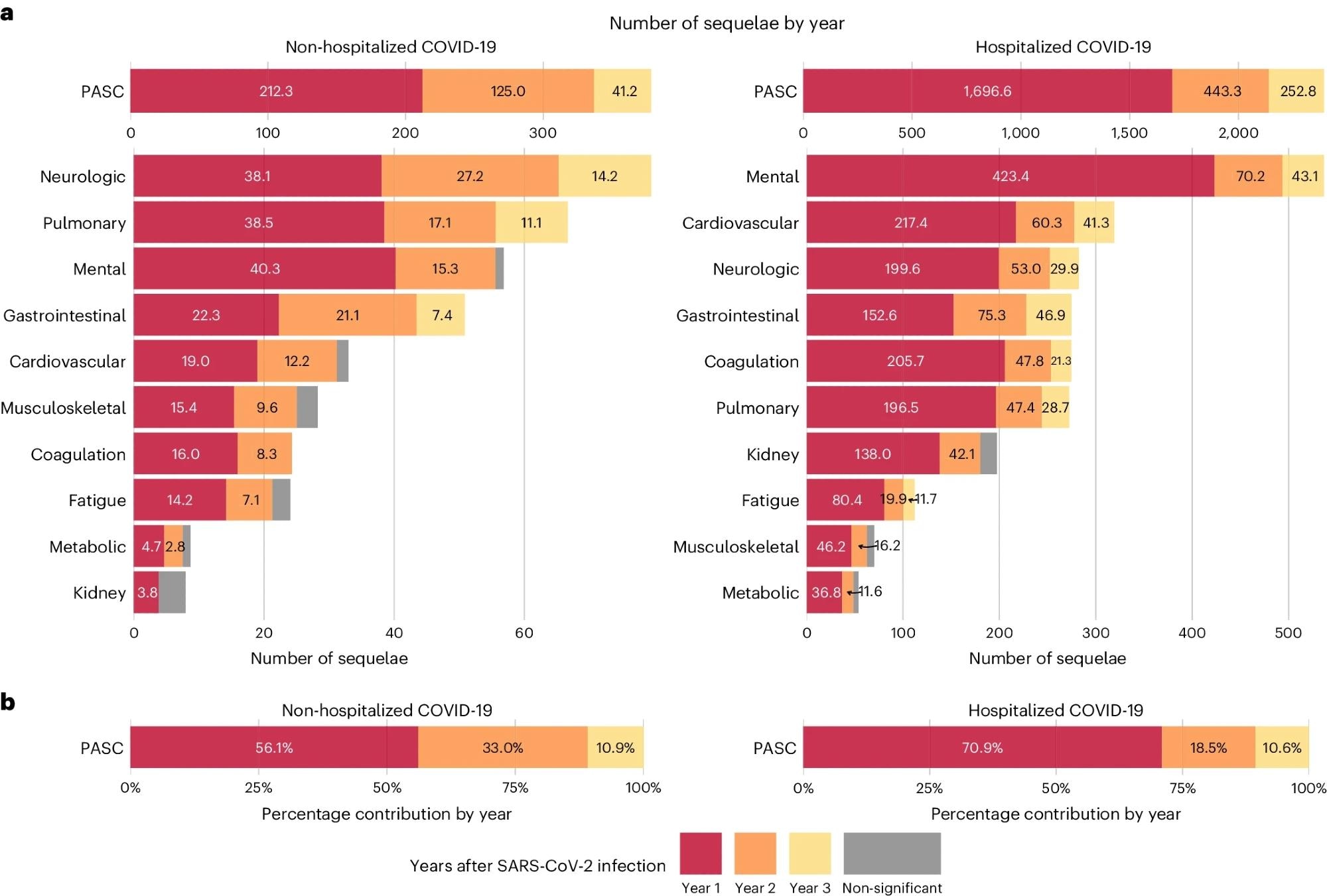 a, Number of post-acute sequelae overall and by organ system per 1,000 persons in the first, second and third year after SARS-CoV-2 infection by care setting of acute phase. b, Relative percentage of number of post-acute sequelae overall in the first, second and third year after SARS-CoV-2 infection by care setting of acute phase. Number of post-acute sequelae for COVID-19 not significantly different from the control group without infection in a year is marked by gray bars. The left column represents numbers of post-acute sequelae for the non-hospitalized COVID-19 group (n = 114,864), and the right column represents the numbers for the hospitalized COVID-19 group (n = 20,297), compared to the control group without infection (n = 5,206,835). Outcomes are ordered from top to bottom by cumulative number of post-acute sequelae at 3 years after infection.
a, Number of post-acute sequelae overall and by organ system per 1,000 persons in the first, second and third year after SARS-CoV-2 infection by care setting of acute phase. b, Relative percentage of number of post-acute sequelae overall in the first, second and third year after SARS-CoV-2 infection by care setting of acute phase. Number of post-acute sequelae for COVID-19 not significantly different from the control group without infection in a year is marked by gray bars. The left column represents numbers of post-acute sequelae for the non-hospitalized COVID-19 group (n = 114,864), and the right column represents the numbers for the hospitalized COVID-19 group (n = 20,297), compared to the control group without infection (n = 5,206,835). Outcomes are ordered from top to bottom by cumulative number of post-acute sequelae at 3 years after infection.
Conclusions
Overall, the study found that the risk of mortality and incident PASC outcomes declined over a three-year follow-up after the initial SARS-CoV-2 infection but remained significant for those individuals who had severe COVID-19 requiring hospitalization.
No new adverse outcomes associated with PASC that had not already manifested were observed over the three-year follow-up. However, the PASC symptoms were still responsible for a significant number of disability-adjusted life years among COVID-19 patients requiring hospitalization.
 Azelastine nasal spray prevents COVID-19 and rhinovirus infections
Azelastine nasal spray prevents COVID-19 and rhinovirus infections