The outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) led to the coronavirus disease 2019 (COVID-19) pandemic, which has claimed over 6.4 million deaths to date. Despite stringent efforts to limit viral transmission, SARS-CoV-2 has spread rapidly and mutated several times. This has led to the emergence of novel SARS-CoV-2 variants with higher transmissibility and immune evasion characteristics.
Study: Dynamics of Competing SARS-Cov-2 Variants During the Omicron Epidemic in England. Image Credit: Mayboon / Shutterstock.com
Introduction
The most recent SARS-CoV-2 variant of concern (VOC) to be described is the Omicron (PANGO lineage B.1.1.529) variant. This variant has many mutations in its spike protein, as well as other viral proteins.
For example, the Omicron variant has 15 mutations in its receptor binding domain (RBD), which binds to the host angiotensin-converting enzyme 2 (ACE2) receptor. These mutations alter the sites where neutralizing antibodies bind to the RBD, subsequently allowing Omicron to escape neutralization, even after vaccination or prior infection with older SARS-CoV-2 variants.
The result has been increasing rates of reinfections and breakthrough infections. However, with decreasing rates of testing coupled with available testing capacity that is currently at 100%, the actual proportions of the Omicron wave remain unknown.
To overcome this challenge, the current study used data from the REal-time Assessment of Community Transmission-1 (REACT-1) study, which is a cross-sectional testing study conducted in England.
Study findings
In the study samples, the Omicron prevalence remained around 0.11% on December 7, 2022, which was about three weeks from the first confirmed case in England. Simultaneously, the Delta variant, which was the dominant circulating strain throughout the preceding three months, had a prevalence of 1.3%.
The Omicron strains appeared to be primarily imported from or exported to the United States, Germany, and France.
About 50% of COVID-19 cases in England were caused by Omicron by the end of the next week. By December 23, 2021, 90% of cases were due to Omicron.
By February 14, 2022, Omicron was responsible for almost all cases. The last Delta-positive sample was also reported on this day.
Omicron cases increased at 0.2 per day from November 23, 2021, to March 1, 2022. On December 3, 2021, which is when the researchers of this study detected the first Omicron case, the growth rate was 0.37. Just over a month later, it was only 0.1.
This might be due to the lower generation time for Omicron, which is estimated to be 28% less than that of the Delta variant. The higher rate of viral spread among younger and less vaccinated age groups who also mixed more in social circles could also be a contributing factor.
By the end of 2021, about 7% of swabs were positive for Omicron; however, this prevalence decreased to less than 5% during January 2022. Later the same month, the rate again increased to about 2.6% by early March 2022.
The reproductive number (Rt) was about two on December 17, 2022, which was two weeks following the onset of the Omicron wave in the U.K. At this time, 90% of those aged 12 and older had been vaccinated with at least one dose of a COVID-19 vaccine, 82% with two doses, and 53% with three doses.
The Rt subsequently declined as social interactions were reduced. By the beginning of January 2022, the Rt was below one.
In late January 2022, the Rt increased to over one and subsequently declined throughout February; however, it tended to rise during this month.
Despite the significantly high levels of recent infections, the herd immunity threshold required for prevalence to decrease had not yet been reached.”
In regards to the general population, the prevalence of Omicron increased throughout England to above 7% in the North East of England. However, its prevalence was less than 4% in East England. London was associated with the earliest peak, which was likely because Omicron was first introduced here.
The Rt was highest in those between the ages of five and 17 years in January 2022. In other age groups, the Rt value quickly dropped below one.
The prevalence of Omicron peaked in this group on January 28, 2022, at almost 11%. This was comparable to less than 8% on January 1, 2022, in those between the ages of 18 and 34.
Individuals aged 55 years or older were associated with the lowest prevalence, which is consistent with their high vaccination rates. Nevertheless, the Rt value in this group increased on March 1, 2022, to 1.1.
This demonstrates the limited vaccine effectiveness of COVID-19 vaccines against Omicron infection.”
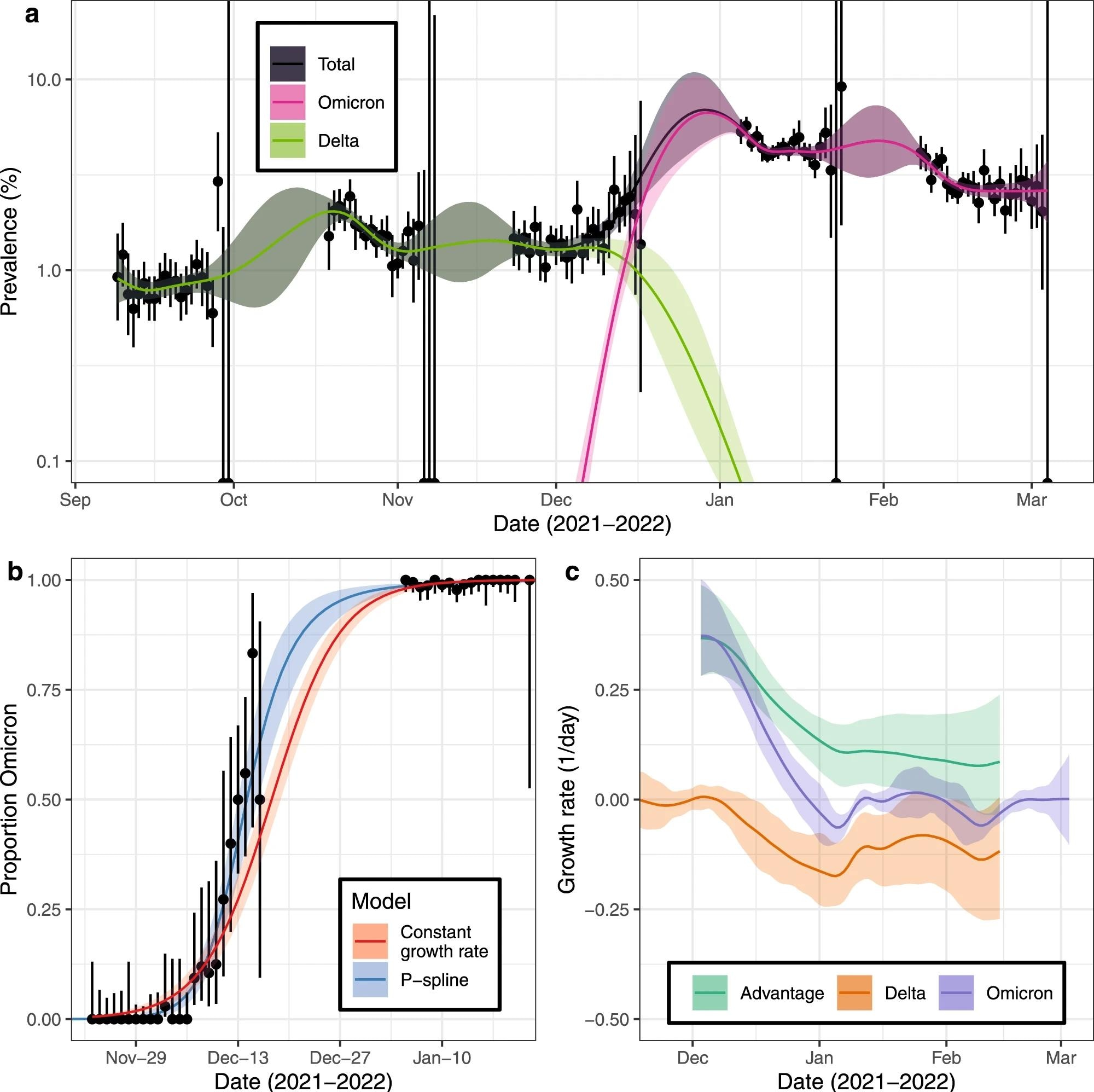
a Modelled prevalence of SARS-CoV-2 variants Omicron and Delta in England estimated using a mixed-effects Bayesian P-spline model. Estimates of prevalence are shown with a central estimate (solid line) and 95% (shaded region) credible intervals. Daily weighted estimates of mean prevalence (points) are shown with 95% credible intervals (error bars). b Modelled proportions of lineages identified as Omicron in England, estimated using Bayesian logistic regression (red) and using a mixed-effects Bayesian P-spline model (blue). Estimates are shown with a central estimate (solid line) and 95% credible intervals (shaded region). Daily estimates of the mean proportion of lineages Omicron (points) are shown with 95% confidence intervals (error bars). c Daily growth rate of Omicron (purple), Delta (orange) and their additive difference (green) estimated from the mixed-effects Bayesian P-spline model. Estimates are shown with a central estimate (solid line) and 95% credible intervals (shaded region).
Sublineage competition
Previous models have shown that Omicron variants BA.1, BA.1.1, and BA.2 showed changing proportions over this period. Even as BA.2 increased, BA.1 prevalence declined.
At the peak of the Omicron wave on December 30, 2021, BA.1 represented 85% of cases as compared to 15% and 0.2% for BA.1.1 and BA.2, respectively.
This trend shifted just two months later, with BA.1 prevalence declining to less than 10% of cases, while BA.1.1 and BA.2 rose to over 20% and nearly 70%, respectively. These variants were responsible for the winter Omicron wave in England.
The daily growth rate of BA.2 and BA.1.1 was 0.133 and 0.42 times higher than that of BA.1, respectively, while BA.1 was 0.09 times higher than BA.1.1. Both variants are more transmissible than BA.1, with BA.2 spreading at the fastest rate of these three Omicron subvariants.
BA.1.1 became dominant in some countries before BA.1 even established itself, thus indicating its superior fitness through a greater number of beneficial mutations.
The Rt for BA.2 was 1.17 as compared to 0.77 for non-BA.2 Omicron variants on March 1, 2022. This supports the replicative fitness of BA.2.
BA.2 is also associated with the most specific COVID-19 symptoms such as anosmia, ageusia, fever, and new long-term cough in a higher proportion of patients as compared to BA.1 infections.
Implications
The current study used high-quality REACT-1 data to estimate the prevalence of Omicron infections. The researchers also describe the exposure risk for Delta and Omicron infections, as well as for BA.1, BA.1.1, and BA.2 separately.
The dynamics of these different variants have been reflected in their different growth rates and prevalence over time, rather than treating them all as a single variant.
Further studies will need to examine whether different lineages and sublineages have different cycle thresholds (Ct) for detection, which could change their observed prevalence. Nonetheless, the study findings demonstrate that SARS-CoV-2 will achieve new levels of fitness through the development of mutations that improve its immune escape characteristics.
"Assuming the emergence of further distinct variants, intermittent epidemics of similar magnitudes [as Omicron, which reached a record prevalence of 7% in England at one point] may become the ‘new normal’.”
Booster vaccine doses and improving current COVID-19 vaccines to provide immunity against these newer variants, as well as continued monitoring, will be essential for maintaining public health.
Journal reference:
- Eales, O., de Oliveira Martins, L., Page, A. J., et al. (2022). Dynamics of Competing SARS-Cov-2 Variants During the Omicron Epidemic in England. Nature Communiations. doi:10.1038/s41467-022-32096-4.
 Large Swedish study finds COVID-19 vaccination unrelated to fertility or childbirth rates
Large Swedish study finds COVID-19 vaccination unrelated to fertility or childbirth rates