Since the onset of the coronavirus disease 2019 (COVID-19) pandemic, which is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), several genetically distinct variants of SARS-CoV-2 have emerged that are more transmissible and virulent than the initial SARS-CoV-2 strain.
 This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Background
In May 2021, the emergence of a new SARS-CoV-2 variant of concern (VOC) known as the Delta variant was announced by the World Health Organisation (WHO). The SARS-CoV-2 Delta variant was first detected in India during September 2020 and quickly became the dominant circulating strain by the Spring of 2021 in many countries around the world.
The Delta variant consists of 30 mutations in the genome that are associated with its increased transmissibility, immune evasion, and higher rates of hospitalization. Three significant mutations observed in the Delta variant include the P681R mutation in the furin cleavage site, L452R mutation in the receptor-binding domain (RBD), and the nucleocapsid mutation R203M.
By the time the Delta variant became the dominant circulating strain in the United Kingdom in May 2021, it was present in a heterogeneous landscape of prior immunity from infection and vaccination, as well as non-pharmaceutical interventions (NPIs).
A new study published on the preprint server medRxiv* examined SARS-CoV-2 genomes that were collected from several random samples during community-based COVID-19 testing in England between March 12 and June 15, 2021. In doing so, the researchers were interested in evaluating the effectiveness of policies that were implemented during this time to reduce international importations and how they contributed to the transmission dynamics of the Delta variant in England. The study also investigated the growth of the Delta variant in both England and the United States (U.S.).
About the study
The current study involved a collection of International (non-U.K.) sequences from GISAID, which were then combined with English sequences as of September 2021. Phylogenetic analyses were carried out to provide an overview of the global expansion of the Delta variant.
A wide range of data was collected for the study that included state-level incidence data from India, incidence data from England, travel history data, COVID-19 case count and vaccination data of the U.K., U.K. population data, state-level COVID-19 case count data of U.S., U.S. states’ population-level immunity, state-level population data from the U.S., global population data, as well as aggregated and anonymized human mobility data.
Finally, estimated importation intensity (EII), estimated exportation intensity (EEI), and estimated local human mobility intensity values were calculated.
Study findings
The results indicated that out of all the international introductions of the Delta variant to England, approximately half originated from India. The majority of the Delta genomes could be traced back to having been introduced before the implementation of mandatory hotel quarantine for people arriving from India.
The EII of the Delta variant to England from India increased significantly in April 2021, following an increase in Delta cases in India, and remained high until May 2021. However, after May 2021, importations from other countries aside from India led to a dominated importation of Delta cases in England.
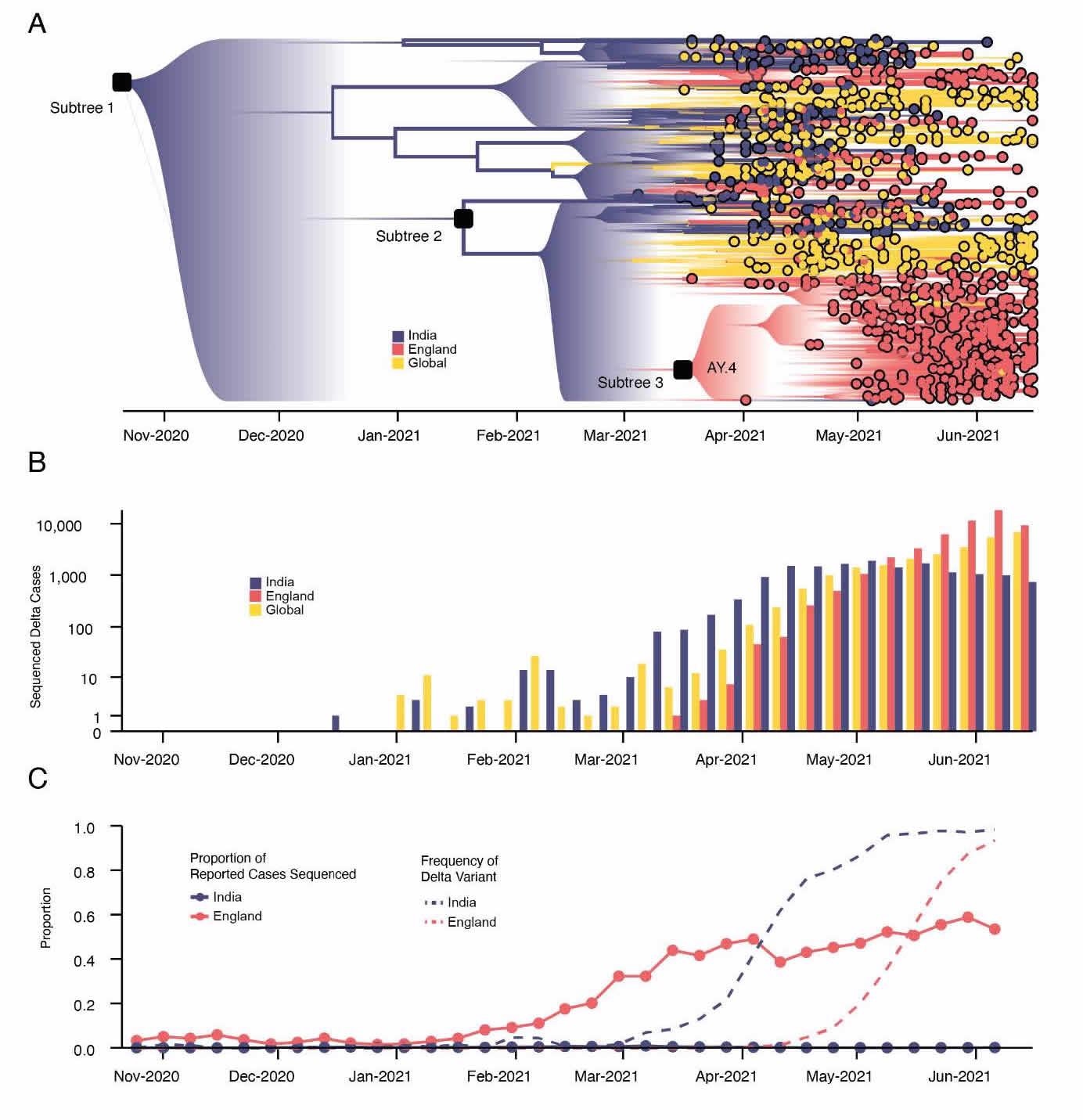
Emergence and rapid geographic expansion of Delta: a) time-calibrated phylogenetic reconstruction of Delta based on 1,000 sequences subsampled from 93,649 sequences from 100 countries (52,992 from England). The tree was split in 3 subtrees (n=28,783, 28,715, and 36,151 sequences) prior to full analysis. The roots of these 3 subtrees, and of lineage AY.4 are labeled. Lineage colors represent the inferred countries and/or regions where transmission occurred. b) Number of sequenced cases of Delta per week in India, England, and the rest of the world. c) Time-varying proportion of sequenced reported positive cases in India and England (solid lines, n = 52,992 sequences are from England, corresponding to 84% of all sequences from the UK) and the proportion of sequenced cases classified as Delta in India and England (dashed lines).
Although hotel quarantine policies were implemented, several additional factors contributed to the onward transmission of this variant within England. For example, a separate terminal for arrivals from mandatory quarantine countries was not opened at airports in the U.K. until June 1, 202. Furthermore, individuals could become infectious and transmit the infection after leaving quarantine, individuals could infect others through connecting flights, and exemptions to hotel quarantine existed.
The results reported that the importations of the Delta variant increased due to the relaxation of social distancing regulations in England. Several lineages of Delta were found to circulate in England such as lineage I, which was sampled mostly in Greater Manchester and Lancashire, lineage II, which was distributed in North West England, lineage III in Greater London and the South East, and lineage V in Bedfordshire.
Delta growth rates were also found to vary across different locations and weeks in England due to heterogeneous levels of mobility and mixing, both local and regional, as well as higher international importations. However, vaccination rates had no major role in the local variation in Delta growth rates in England. In the case of the United States, where levels of immunity through infection and vaccination varied, higher baseline local immunity levels were found to be associated with a higher overall growth of Delta.
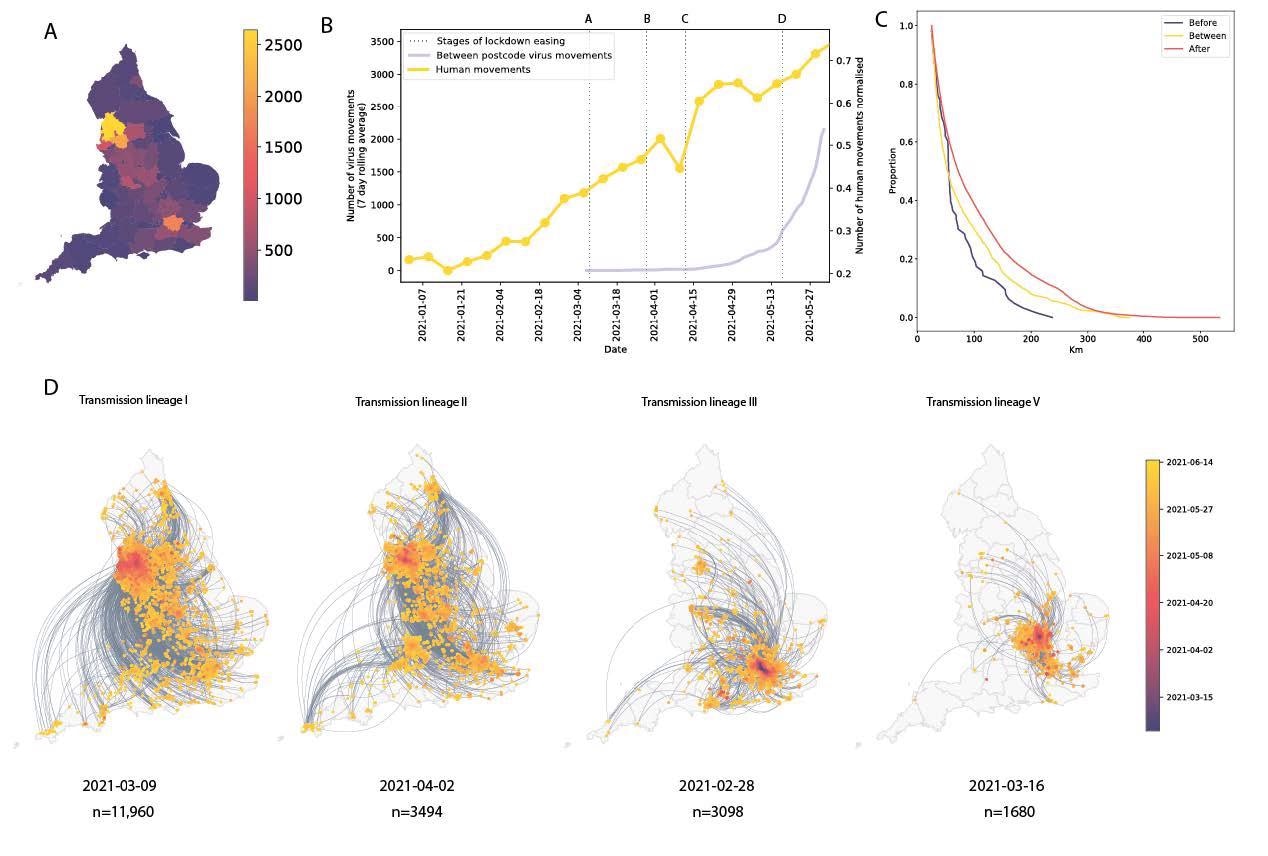
Introductions and regional dynamics of Delta transmission lineages. a) Number of independent introductions per UTLA in England based on continuous phylogeographic analysis of all Delta transmission lineages with >5 sequences. b) Trends in aggregate human mobility and the number of virus lineage movements among postcode districts. Letters denote stages of lockdown easing: A (2021- 03-08) schools reopen and limited mixing between households outdoors permitted; B (2021-03-29) “Stay at home” directive lifted, more outdoor mixing allowed (up to six people from two households; C (2021- 04-12) non-essential retail re-opened, outdoor dining permitted, holiday lets and campsites re-open; D (2021-05-17) indoor hospitality opens, indoor mixing permitted. c) Proportion of virus lineage movements between postcodes >25 km apart: y-axis denotes the proportion of movements that are less than or equal to the value on the x-axis. This is shown for movements before lockdown easing on 12th April (blue), between 12th April and 17th May (yellow) and after 17th May (red). d) Virus lineage movements inferred by continuous phylogeographic analysis for four large transmission lineages (see transmission lineages IV-VII in Extended Data Fig. 5). Direction of lineage movement is anti-clockwise, and dots represent the start and end points of movement, coloured by inferred date. The size and inferred TMRCA of each lineage is shown below each map.
Conclusions
The current study, therefore, demonstrates that higher Delta growth rates were positively associated with levels of local mixing in England, as well as levels of population immunity and vaccination in the United States. However, the existence or magnitude of NPIs must be maintained in order to provide relief to the healthcare burden of the Delta variant.
Further research must be carried out to assess the factors that are conducive to the spread of SARS-CoV-2 variants in particular contexts so that appropriate responses could be planned promptly and appropriately.
This news article was a review of a preliminary scientific report that had not undergone peer-review at the time of publication. Since its initial publication, the scientific report has now been peer reviewed and accepted for publication in a Scientific Journal. Links to the preliminary and peer-reviewed reports are available in the Sources section at the bottom of this article. View Sources
Journal references:
- Preliminary scientific report.
McCrone, J. T., Hill, V., Bajaj, S., et al. (2021). Context-specific emergence and growth of the SARS-CoV-2 Delta variant. medRxiv. doi:10.1101/2021.12.14.21267606. https://www.medrxiv.org/content/10.1101/2021.12.14.21267606v1.
- Peer reviewed and published scientific report.
McCrone, John T., Verity Hill, Sumali Bajaj, Rosario Evans Pena, Ben C. Lambert, Rhys Inward, Samir Bhatt, et al. 2022. “Context-Specific Emergence and Growth of the SARS-CoV-2 Delta Variant.” Nature 610 (7930): 154–60. https://doi.org/10.1038/s41586-022-05200-3. https://www.nature.com/articles/s41586-022-05200-3.
 COVID-19 severity is linked to changes in mitochondrial DNA methylation
COVID-19 severity is linked to changes in mitochondrial DNA methylation