Among the different SARS-CoV-2 variants of concern (VOCs), the severity of Coronavirus disease 2019 (COVID-19) in adults is high, while children and young adults are not as severely impacted. Furthermore, various other viruses such as the Middle Eastern respiratory syndrome coronavirus (MERS-CoV), herpes family viruses, and flavivirus have been found to cause mild to no symptoms in children.
About the study
The present study aimed to summarize the various manifestations of SARS-CoV-2 in children and presented possible mechanisms for the same. In addition, the research also discussed the resource allocation theory to explain the different effects of COVID-19 in children.
Severe SARS-CoV-2 infections in children of ages averaging two, six, and nine years were the focus of this work. At the COVID Human Genetic Effort consortium, patients with autoimmune polyendocrine syndrome type 1 (APS1) were studied and it was observed that these patients carry neutralizing autoantibodies to various cytokines, including interferons type-I (IFN-I) and interleukin-17 (IL-17) cytokines. The ability of these autoantibodies to phenocopy inborn errors of IFN-I and their role in causing severe SARS-CoV-2 infections was also investigated.
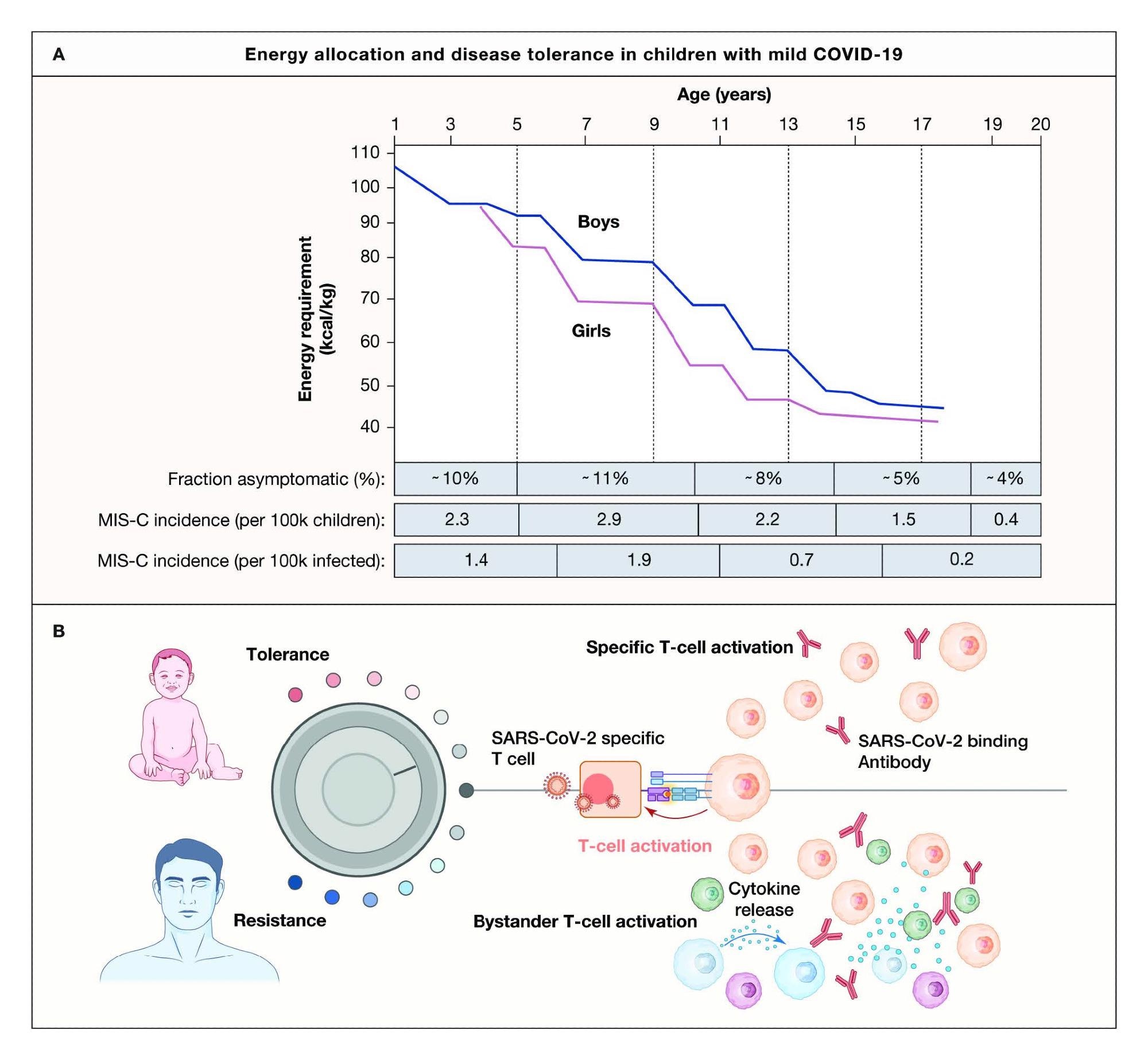
An energy allocation theory to explain mild COVID-19 and MIS-C in children based on disease tolerance and viral persistence. (A) Energy requirement (kcal/kg) decreases with age in US children and is slightly higher in boys than girls (adapted from Torun B, Pub. Health. Nutr, 2005). The fraction of asymptomatic children among SARS-CoV2 PCR+ children across the indicated age groups (Leidman et al, 2020), MIS-C incidence in the US per 100k children across indicated age groups (Belay et al, 2021), and MIS-C incidence per 1 million cases of COVID-19 across the indicated age groups (Payne et al, 2021). (B) In growing children, the threshold for energy-expenditure on system inflammatory responses are higher, leading to disease tolerance in most cases and mild to asymptomatic COVID-19, while in the elderly, the obese, and individuals with inadequate type-I IFNrespones, systemic inflammation is triggered, driving bystander T cell activation and immunopathology.
Results
The study results show that individuals under 50 years with severe COVID-19 manifestations had inborn genetic errors in toll-like receptor 3 (TLR3) or an essential inducer of Type I IFN called gene interferon regulatory factor 7 (IRF-7). Deficiencies in the type-I IFN receptor, interferon-alpha and beta receptor subunit 1 (IFNAR1), and X-linked viral sensor toll-like receptor 7 (TLR-7) were also observed in severe COVID-19 patients. Mild to asymptomatic COVID-19 was detected in patients with defective B cells, T cells, or both.
Notably, children with APS1 were more vulnerable to developing very severe COVID-19. Also, after screening the sera of patients with severe COVID-19, approximately 2.6% of females and 12.5% males carried neutralizing autoantibodies to IFN-I. Moreover, neutralizing autoantibodies to IFN-I was present in more than 6% of individuals above 80 years of age and accounted for almost 20% of deaths related to severe COVID-19. The study found that SARS-CoV-2 can influence IFN-I responses as the virus encodes multiple proteins associated with the IFN-I gene. Innate immune responses like type-I/II IFN-responses in the upper airway were observed to be more distinct in SARS-CoV-2-infected children than in infected adults.
Severe COVID-19 is characterized by distinctive T cell lymphopenia, robust B cell activation, T cell activation, and higher production of neutralizing antibodies as compared to mild COVID-19. SARS-CoV-2-specific immunoglobulin A (IgA) antibodies were observed in adults with severe COVID-19, while these were not present in children suffering from mild COVID-19.
Conclusion
Based on findings by the COVID Human Genetic Effort consortium, the study concluded that the development of an antiviral type-I IFN immunity early after COVID-19 infection in individuals could determine the extent of severity of COVID-19 in the individual. The number of autoantibodies to IFN-I was found to be proportional to an increase in age in patients with severe COVID-19 infections. Therefore, the study results support the removal of neutralizing anti-IFN-I autoantibodies using plasma exchange to treat children with APS-1 infected with SARS-CoV-2.
Failure of early IFN-I and/or IFN-III responses to control the replication of SARS-CoV-2 leads to severe COVID-19 complications. Genetic changes in the type I IFN gene explain the occurrence of severe COVID-19 pneumonia in children and young adults. Moreover, the distinctions in tissue immune cell composition and basal antiviral gene expression in epithelial cells between children and adults prove that the antiviral responses in children are much more robust. Understanding the role of local tissue responses in determining the severity of COVID-19 disease will require in-depth research.
The study hypothesizes that in a trade-off between allocating energy to combating a pathogen or promoting growth, a child’s body is more likely to choose the former as the young body builds up its new defenses. Therefore, the immune response in children is bound to select disease tolerance and defense to avoid bodily harm. Among all the immune responses, characteristics like fever, muscle ache, and other signs of systemic inflammation require the most energy. In the case of SARS-CoV-2 infections, children with the highest energy requirements were observed to be asymptomatic. This observation implies that defense mechanisms in children choose to develop a tolerance to the diseases rather than resist them.
 Prenatal wildfire smoke exposure linked to higher autism risk in children
Prenatal wildfire smoke exposure linked to higher autism risk in children