I have the honor of serving as the Head of Therapeutics Development at the Bill & Melinda Gates Medical Research Institute. I joined the institute a little over three years ago, following leadership roles in the pharmaceutical industry and at the CDC.
My career has focused on infectious diseases, and I have spent decades working on TB. My work on TB started after I left medical school, having “learned” that TB was a disease of the past. However, when I moved to Atlanta in 1992 to start my residency training in the city’s extensive public hospital system, I saw that was far from the case. In that urban setting, I cared for many patients suffering from TB, which was steadily increasing due largely to the growing HIV epidemic in the city and the US more broadly.
I then trained in applied epidemiology in the Epidemic Intelligence Service (EIS) at the CDC in the mid-1990s, where I learned that TB remained one of the major infectious diseases killers worldwide, especially in low- and middle-income countries (LMICs). In my training, I focused on combatting the global TB epidemic, and later as permanent staff, I worked on global TB control projects as part of a broader US Government response to the global HIV and TB epidemics.
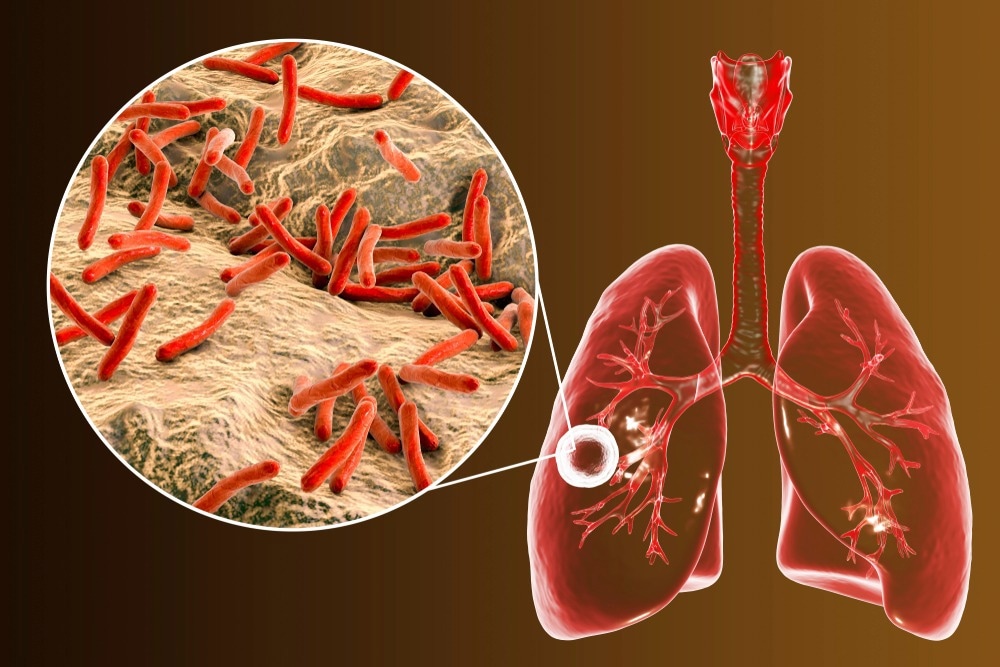
Image Credit: Kateryna Kon/Shutterstock.com
TB is the second leading infectious killer after COVID-19, killing 1.5 million people in 2020 alone. Why is TB so prevalent worldwide, and what current treatment options are available?
Up to a quarter of the world’s population is thought to be latently infected with TB. In 2020 alone, an estimated 10 million people developed active TB— including 1.1 million children— and 1.5 million people died from TB, including an estimated 214,000 people living with HIV. The disease burden remains greatest in LMICs, which account for 98% of reported TB cases.
Prior to the advent of the COVID-19 pandemic, TB was the leading cause of death from a single infectious agent. The COVID-19 pandemic and the resulting strain on health service delivery has accentuated the TB burden, with access to care and case notifications decreasing sharply in 2020 and the number of TB deaths increasing.
Currently, bacille Calmette-Guérin, known as BCG, is the only licensed TB vaccine. However, it has limited impact on preventing Mtb infection and TB disease in adults. Treatment of TB disease is curative but lengthy, and compliance is often incomplete. The global prevalence of drug-resistant TB is substantial. Improved prevention tools and effective vaccines to prevent the development of TB disease are urgently needed to accelerate progress toward ending the TB epidemic. However, since the introduction of the BCG vaccine in 1921, very few novel vaccine candidates have advanced into clinical efficacy trials.
Many people believe TB is in the past and do not see this as a current global threat. Why is this, and how can we help address some misconceptions surrounding this disease?
TB is a disease of the poor, and unfortunately, TB research has experienced research funding shortfalls for decades. In addition, the biology of TB is complex, and our understanding of the organism, TB pathogenesis, and immunology remains limited in support of vaccine design and development. These challenges are not easily overcome. Basic research needs to catch up.
The World Health Organization (WHO) has recently released new guidelines as well as a new operational handbook on tuberculosis care and support. Please tell us more about these new guidelines and what they mean for people living with TB?
The new guidelines on TB care and support are intended to improve the quality of life and lead to better outcomes for people with TB. They include implementation guidance on health education, counseling, and palliative care as well as on social support, treatment administration options, and digital adherence technologies. The guidelines include new 4-month (all oral) treatment regimens – the first advance in shortening and improving treatment for drug-sensitive TB in decades.
Recent clinical evidence informed the new guidelines, which allow for the programmatic implementation of treating almost all forms of drug-resistant TB with either BPaLM (a combination of bedaquiline, pretomanid, linezolid, and moxifloxacin) or BPaL (bedaquiline, pretomanid, and linezolid).

Image Credit: MOUii/Shutterstock.com
Why is it vital that people suffering from TB receive adequate care and support?
As I mentioned earlier, TB is a disease of the poor, and many LMICs do not have adequate infrastructure to support patients fully. Treatment of TB differs from the treatment of many other common diseases, which follow a pathway of diagnosis, a prescription for a course of treatment, and a follow-up visit. In the case of TB, treatment takes a minimum of 6 months and requires ongoing patient engagement, including directly observed therapy for 5-6 days per week in a clinical setting, to support patient adherence and mitigate the risk of spreading the infection.
Treatment enablers such as transport to clinical facilities, taking the drugs with food, and other support is important for TB patients and often challenging to deliver in LMICs. Lastly, patients can sometimes feel better after 3-5 weeks of treatment, leading to poor compliance over the course of the required 6-month treatment period.
Despite new guidelines being released, information usually shared is complex and difficult for the general public to understand. Why is it essential that these guidelines are also provided in easy language? How could governments, policymakers, and organizations make scientific information more digestible to the general population?
The new guidelines are written to help medical professionals and those working in public health. With these latest guidelines, the WHO did an excellent job distilling the salient messages from the update and focused on what is most meaningful and important in TB programs — delivering the treatment and care services to patients and the outcome for the patients.
This 2022 update is concise and straightforward regarding key points, improving further on the 2017 update, which some healthcare professionals perceived as heavy on technical details.
You are currently the head of therapeutics development at Gates MRI. What are some of the current projects underway at Gates MRI concerning TB?
The institute is supporting and investing in multiple vaccines and therapeutics programs. These include the development of novel vaccine interventions to prevent TB and the establishment of global clinical trial capabilities to support future novel approaches to TB control.
The institute’s TB vaccine program has a workstream focused on developing a candidate vaccine, M72/AS01E-4 (under an exclusive license with GSK), for preventing tuberculosis disease in adolescents and adults. In a phase 2b proof-of-concept clinical study (conducted by GSK with support from Aeras), the investigational vaccine demonstrated potential in preventing TB disease among Mtb infected individuals. The first clinical trial Gates MRI has initiated with M72/AS01E-4 is a trial in South Africa to evaluate the safety and immunogenicity of the vaccine candidate in people living with HIV, referred to as the MESA-TB trial (supported by both The Bill & Melinda Gates Foundation and The Wellcome Trust).
In anticipation of a phase 3 trial efficacy trial of the investigational vaccine, the institute is conducting a TB epidemiology study to document the prevalence of latent Mtb infection and the incidence of TB disease in populations with a high TB disease burden. The study also intends to build the required clinical trial capacity to support the investigational vaccine’s phase 3 trial evaluation.
Image Credit: Novikov Aleksey/Shutterstock.com
As well as your current research into potential TB vaccines, Gates MRI is currently involved in revaccination efforts in low-and-middle-income countries. Please can you tell us more about these efforts and the importance of revaccination, especially in low-income countries?
Another of the institute’s current TB research programs, the BCG revaccination clinical trial, is underway in South Africa.
BCG vaccination is commonly given to babies in the first week of life, protecting children from TB for at least ten years, but protection against TB in adolescents and adults is limited. The study has enrolled children and adolescents to assess whether a second dose of BCG vaccine at 10 to 18 years of age helps protect against Mtb. The study follows participants over four years, testing for Mtb infection every six months. If results are favorable, the goal is to implement policy change in countries with a high burden of TB. The study will also examine the immune response to Mtb infection and may help us understand mechanisms of protection and develop new TB vaccines.
What do you believe the future of TB looks like? Are you hopeful we will one day see TB eradicated with continued research, support, and funding?
TB can be preventable and curable with the right investments and resources, and although there is progress in the development of new TB diagnostics, drugs, and vaccines, this is constrained by the overall level of R&D investment. With continued investment, both monetary and scientific, I am confident that a world without TB is attainable.
What is next for you and your research at Gates MRI? Are you involved in any exciting upcoming projects?
The institute is a member of the Project to Accelerate New Treatments for Tuberculosis (PAN-TB) collaboration (the collaboration comprises Evotec, GlaxoSmithKline, Janssen, Otsuka, TB Alliance, the Bill & Melinda Gates Medical Research Institute, and the Bill & Melinda Gates Foundation). This group of philanthropic, non-profit, and private sector organizations is working together to expedite the development of a pan-TB regimen: a novel TB regimen capable of treating nearly all TB patients, even those with drug-resistant forms, to enable a simpler “test and treat” paradigm.
Within the collaboration, Gates MRI is responsible for executing the Phase 2b/2c clinical trials intended to evaluate promising new regimens constructed with TB drugs from the PAN-TB partners to identify the best regimen for subsequent Phase 3 evaluation in close coordination and joint governance with the partners.
A pan-TB regimen that is expected to be significantly shorter than current standard TB treatments (2-3 months) would allow more TB patients to be cured, resulting in less transmission of infection and a reduced burden on health systems that treat TB; this would permit more resources to be focused on finding the estimated 3 million cases of active TB that are often underreported and go undiagnosed and untreated every year. All of these advancements would collectively result in greater global health impacts, with an accelerated decline in TB disease burden that ultimately paves the path to eliminating TB.
Where can readers find more information?
Please visit the institute’s website at gatesmri.org and follow us on Twitter @GatesMRI and on LinkedIn at https://www.linkedin.com/company/bill-melinda-gates-medical-research-institute.
About Charles Wells
I have dedicated my career to addressing global health issues and working to bring forward critically needed new products and tools to address unmet medical needs for TB, HIV, malaria, and other neglected infectious diseases.
My training and experience working in global health to combat the HIV and TB epidemics in low-and-middle-income countries (LMICs) for more than a decade in my earlier career have provided an important and unique framework for my efforts to successfully develop commercial products for neglected infectious diseases.
Through the course of this work, I have led large and diverse mission-driven teams of local and international-based staff; managed complex partnerships, budgets and funding streams; mentored numerous young professionals in infectious diseases, public health and pharmaceutical product development; and translated my experience and efforts into measurable impact on global health.
 Early tuberculosis treatment reduces sepsis deaths in HIV patients
Early tuberculosis treatment reduces sepsis deaths in HIV patients